Volume 24, Number 7—July 2018
Research
Molecular Epidemiology of Human Adenovirus–Associated Febrile Respiratory Illness in Soldiers, South Korea1
On This Page
Jung Yeon Heo2, Ji Yun Noh2, Hye Won Jeong, Kang-Won Choe, Joon Young Song, Woo Joo Kim, and Hee Jin Cheong
Abstract
During January 2013–April 2014, we subjected nasopharyngeal specimens collected from patients with acute febrile respiratory illness in a military hospital to PCR testing to detect 12 respiratory viruses and sequence a partial hexon gene for human adenovirus (HAdV) molecular typing. We analyzed the epidemiologic characteristics of HAdV infections and compared clinical characteristics of HAdV types. Among the 305 patients with acute febrile respiratory illness, we detected respiratory viruses in 139 (45.6%) patients; HAdV was the most prevalent virus (69 cases). Of the 40 adenoviruses identified based on type, HAdV-55 (29 cases) was the most prevalent, followed by HAdV-4 (9 cases). HAdV-55 was common in patients with pneumonia (odds ratio 2.17; 95% CI 0.48–9.86) and hospitalized patients (odds ratio 5.21; 95% CI 1.06–25.50). In soldiers with HAdV infection in Korea, HAdV-55 was the most prevalent type and might be associated with severe clinical outcomes.
Human adenoviruses (HAdVs) are considered the most important causative agent of acute respiratory infection in soldiers, particularly in new recruits (1,2). A total of 79 HAdV types have been documented (3). The distribution of HAdV types differs substantially by geographic region and environmental factors (4,5). HAdVs are prevalent in training facilities or military barracks for soldiers, but the prevalent types of HAdV have changed over time (6). Historically, HAdV-4 and HAdV-7 were the most prevalent causes of acute febrile respiratory illness (AFRI) among US military personnel since the 1950s (7). Vaccination against HAdV-4 and HAdV-7 has been effective in reducing AFRI among US military trainees to date (8,9). However, since 2007, the emergence of new adenovirus types such as HAdV-14, which is distinct from the prototype in the United States, has been associated with outbreaks of AFRI and severe pneumonia (including several deaths) in military populations (10,11).
HAdV is most prevalent in patients with acute lower respiratory tract infection and is the most common cause of pneumonia among military personnel in South Korea (12). However, studies evaluating the types of HAdVs in this population are limited because of the lack of knowledge about HAdVs among military physicians. In 2012, HAdV-55 was identified in patients with severe pneumonia, and an outbreak of AFRI among military personnel in South Korea was recorded (13,14). HAdV-55, which is a novel HAdV type characterized by genome recombination between HAdV-B11 and HAdV-B14, caused outbreaks of acute respiratory diseases in military camps in Turkey, China, and Singapore (15–18). Although the cases of pneumonia caused by HAdV-55 among military personnel in South Korea have been recorded, information on the epidemiology and characteristics of type-specific HAdV respiratory infections among military personnel in South Korea is limited. Thus, our study aimed to investigate the epidemiology of HAdVs infections and to compare the clinical characteristics by type of HAdVs in soldiers in South Korea via hospital-based surveillance on viral respiratory infections.
Characteristics of the Study Population and Case Definition
The study was approved by the Institutional Review Board of the South Korea Armed Forces Medical Command. During January 2013–April 2014, we enrolled in the study all new recruits and active duty soldiers with AFRI who were required to visit the emergency department or to undergo hospitalization at the Armed Forces Capital Hospital in Seongnam, South Korea. We defined AFRI as a history of fever or measured fever >37.6°C and the presence of >1 respiratory symptom such as cough, sore throat, or rhinorrhea with onset within the last 7 days. The Armed Forces Capital Hospital is the only tertiary care hospital in the South Korea military healthcare system. Furthermore, the hospital offers primary and secondary medical services to soldiers in the city of Seoul and Gyeonggi Province. Almost all soldiers in South Korea, except officers, use military hospitals for free health services.
Respiratory Virus Multiplex Reverse Transcription PCR
We collected nasopharyngeal or throat swab specimens from the patients with AFRI within 24 hours after their hospital visit by using a flocked swab. We stored the specimen at 4°C in viral transport media until further testing. Within 3 days of collection, we sent specimens to a commercial laboratory center (GC Labs, Yongin, South Korea), where they were subjected to respiratory virus multiplex reverse transcription PCR.
We extracted total viral nucleic acid from the specimen by using the Chemagic Viral DNA/RNA Extraction Kit (Chemagen Inc., Baesweiler, Germany) and performed cDNA synthesis by using the CapFishing Full-Length cDNA Premix Kit (Seegene Inc., Seoul, South Korea). We performed PCR by using the Seeplex RV12 ACE Detection Kit (Seegene Inc., South Korea), which is used for identifying influenza viruses A and B, respiratory syncytial viruses A and B, adenovirus, parainfluenza virus types 1–3, rhinovirus group A, human coronavirus 229E/NL63, human coronavirus OC43, and human metapneumovirus.
Molecular Analysis of HAdVs
We extracted DNA from the adenovirus-positive respiratory specimens by using the QIAamp DNA Blood Mini Kit (QIAGEN, Hilden, Germany). We amplified the partial nucleotides of the hexon gene by using PCR as described elsewhere with some modifications (19). We amplified viral sequences by using oligonucleotide primers producing a 475-bp fragment: ADHEX1F (5′-CAACACCTAYGASTACATGAA-3′) and ADHEX1R (5′-KATGGGGTARAGCATGTT-3′). PCR conditions were as follows: initial denaturation at 94°C for 1 min, followed by 35 cycles of denaturation at 94°C for 1 min, annealing at 50°C for 1 min, elongation at 68°C for 1 min, and final extension at 68°C for 5 min. For samples that tested negative in the first PCR reaction, we performed heminested PCR by using primers (273 bp) ADHEX1F (5′-CAACACCTAYGASTACATGAA-3′) and ADHEX2R (5′-ACATCCTTBCKGAAGTTCCA-3′) with the same temperature and time profiles. We determined DNA sequences in both directions by using the Applied Biosystems Automatic Sequencer ABI 3730xl and ABI Prism BigDye Terminator v3.1 sequencing system (Applied Biosystems, Foster City, CA, USA). We identified the type of HAdV by using BLAST (http://blast.ncbi.nlm.nih.gov/Blast.cgi).
We generated phylogeny on the basis of the 232-bp nucleotide sequences of the hexon gene of HAdVs. For the phylogenetic analysis, we selected the sequences of each type of HAdV from GenBank. We used MEGA 6 software to generate the phylogenetic tree and evaluated topologies by performing a bootstrap analysis of 1,000 iterations (20).
Collection of Clinical Data
We obtained clinical information of the patients with HAdV respiratory infection during the study period from standardized case report forms. The case report forms, which included clinical diagnosis, intensive care unit stay, requirement for mechanical ventilation or vasopressor, and symptoms at presentation, were completed within 7 days from the hospital visit by an attending physician.
Statistical Analysis
We conducted Pearson’s χ2 and Fisher exact test for the demographic and clinical variables by using the SPSS for Windows version 20 (IBM Corp., Armonk, NY, USA). For all analyses, we defined statistical significance as p<0.05.
Epidemiology of HAdVs in Soldiers with AFRI
During January 2013–April 2014, we enrolled 305 patients with AFRI in the study. We detected a total of 157 respiratory viruses in 139 (45.6%) soldiers with AFRI. HAdV was the most prevalent virus (49.6% [69/139]), followed by influenza A or B virus (28.8% [40/139]) and rhinovirus group A (12.2% [17/139]). Among 139 cases in which respiratory viruses were identified, >2 viruses were detected in 18 cases (12.9%) (Table 1).
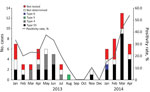
Figure 1. Temporal distribution of acute febrile respiratory illness from human adenovirus (HAdV) infection among soldiers (no. cases) and overall HAdV positivity rate among collected specimens, by HAdV type, South Korea, January 2013–April...
We commonly observed cases of HAdV infection during winter and spring (Figure 1). Among the tested cases of AFRI, the monthly positive rate for HAdV ranged from 0% to 53.8%; average positivity rate was 22.6%. A peak positive rate for HAdV infection occurred in soldiers with AFRI during March–April 2014. The mean age of the patients with HAdV infection was 21.7 years. Among the 69 patients with HAdV infection, 40.6% were new recruits and 75.4% were hospitalized (Table 2).

Figure 2. Phylogenetic tree human adenoviruses detected among soldiers with acute febrile respiratory illness from human adenovirus (HAdV) infection, South Korea, January 2013–April 2014. Tree was constructed by the neighbor-joining method on the...
From the 69 patients with HAdV infection, 51 respiratory specimens were available for further molecular analysis. For the 51 samples tested, we identified the HAdV type in 40 samples (Figure 2). HAdV-55 (72.5% [29/40]) was the most prevalent type in soldiers with HAdV infection, followed by HAdV-4 (22.5% [9/40]). We detected HAdV-55 and HAdV-4 in 2013, but we did not detect HAdV-4 in 2014. We detected HAdV-5 and HAdV-6 in 1 case each.
Clinical Characteristics of HAdV-55 Infection versus Other Types of HAdV Infections
We observed no statistically significant difference in the demographic characteristics or signs and symptoms of the patients with HAdV-55 infection compared with those with other types of HAdV infection (Table 3). Furthermore, we observed no statistically significant difference between the patients in terms of laboratory and radiographic findings. Co-infections with other bacteria or viruses were similar in both groups. The patients with HAdV-55 infection were more likely to have onset pneumonia (44.8% vs. 27.3% [odds ratio (OR) 2.17; 95% CI 0.48–9.86]) and be hospitalized (86.2% vs. 54.5% [OR 5.21; 95% CI 1.06–25.50]) than those infected with other types of HAdV. In particular, we identified HAdV-55 infection in all patients who required hospitalization in the intensive care unit or mechanical ventilation caused by acute respiratory distress syndrome (ARDS).
In our study, HAdV was the most prevalent virus detected among soldiers with AFRI in South Korea, representing 49.6% of the cases. HAdV-55 was the most prevalent type among the cases that could be identified using PCR. Although HAdV-55 has recently received public attention as an emerging pathogen that causes outbreaks of respiratory illness and severe pneumonia in the general population and soldiers, acute respiratory illness associated with HAdV-55 has rarely been reported in the civilian population in South Korea (6,16,21–23). In children in South Korea, HAdV-3 and HAdV-7 are prevalent serotypes and have also been associated with the outbreaks of adenoviral respiratory illness since the 1990s (24,25). Severe pneumonia cases associated with HAdV-55 infection were recently reported in soldiers in South Korea (13,14). Our finding that HAdV-55 was the most prevalent type in soldiers in South Korea differs from the epidemiology of adenovirus in children in South Korea.
Another notable finding of this study was the changing epidemiologic trend from the co-circulation of HAdV-4 and HAdV-55 in 2013 to the predominant circulation of HAdV-55 in 2014. HAdV-4 was the second most common type after HAdV-55 among soldiers with AFRI in South Korea in 2013. However, HAdV-4 has not been identified in soldiers in South Korea since November 2013. Although the shift in the HAdV types in soldiers in South Korea could not be fully understood because of the relatively short study period, HAdV-55 infection has been prevalent among soldiers in South Korea since 2014 (14,26).
Pneumonia and hospitalization associated with HAdV-55 infection were more frequent than those associated with the other types of HAdV infection in soldiers in South Korea. In particular, HAdV-55 infection was associated with severe pneumonia or ARDS. Nevertheless, we observed no significant differences between HAdV-55 cases and non–HAdV-55 cases in terms of the frequency of clinical diagnosis of pneumonia, hospitalization, and ARDS. These findings could be explained by 2 assumptions. First, specific HAdV types such as HAdV-3, HAdV-7, or HAdV-14 might be more virulent than other types (25,27,28). Considering that the HAdV-55 genome is more similar to the HAdV-14 genome than the HAdV-11 genome, HAdV-55 infection could be associated with severe respiratory infection in certain patients (17). Second, the lower levels of herd immunity against HAdV-55 could have an influence on the epidemic of HAdV-55–associated respiratory infection in soldiers in South Korea (29,30). Severe respiratory illness and outbreaks associated with HAdV-55 in soldiers in South Korea might be similar to those observed in military personnel in China (13,14,21,22).
In this study, the proportion of new recruits with HAdV infection among soldiers in South Korea was not as high as expected. More than half of the South Korean soldiers with HAdV infection were on active duty. These findings contrast with previous data in which HAdV-associated respiratory infection has been common among new recruits (7). The patients included in this study might have had clinically severe illness rather than mild illness because our institute is the only central referral hospital in the military system in South Korea. Moreover, HAdV easily spreads to advanced training sites or military barracks and it can spread in geographically dispersed military barracks by the movement of soldiers because of prolonged viral shedding (31). In this study, some of the patients with HAdV-55 infection who were active duty soldiers were identified in the clusters of patients in 4 military barracks (data not shown). Although the outbreak of HAdV-55 infection was not directly confirmed in this study, outbreaks of HAdV-55–associated respiratory infection might be occurring among active duty soldiers.
Our study has some limitations. First, the study was performed for a relatively short period (16 months). Although the data might be insufficient to reflect the epidemiology of respiratory HAdV infection among military personnel in South Korea, the variation of HAdV type over time and the impact of the emergence of HAdV-55 on clinical severity can be observed. Considering the long-term experience of the US military with respiratory HAdV infection, the distribution of HAdV types might show a substantial difference in the military and community populations in South Korea. Thus, a surveillance system must be established to detect the circulation of the HAdV type among military personnel. Second, the study population included patients who needed hospitalization or an emergency department visit. Among soldiers in South Korea with HAdV infection, patients who had severe clinical signs and symptoms might be those who were primarily enrolled in this study. Nevertheless, our results suggest that of the several HAdV types, HAdV-55 and HAdV-4 might be implicated in HAdV respiratory infections among soldiers in South Korea. Furthermore, active duty soldiers and new recruits could have a substantial disease burden caused by respiratory HAdV infection. Third, we could not determine HAdV types in 11 cases. The viral titer in the clinical specimen might have been low and the viral DNA degraded because some respiratory specimens were not frozen until the molecular experiment. Using the 2-step hemi-nested PCR, we did not observe a DNA band in 11 samples.
This study is important because it is a prospective study on patients with AFRI. Studies on the HAdV type in soldiers in South Korea since 2012 are limited. However, the previous studies provided data on the epidemiology of the HAdV type in patients with severe clinical manifestations or in those with HAdV respiratory infection. These conditions might result in bias in the epidemiology of HAdV infections among military personnel in South Korea.
In conclusion, our study found that HAdV was the most prevalent virus among soldiers with AFRI in South Korea. In particular, HAdV-55 and HAdV-4 were the prevalent types in soldiers with HAdV-associated respiratory infection. HAdV-55 was associated with severe clinical outcomes. Further studies are needed to verify which HAdV types are associated with AFRI in military recruits. In addition, studies on the introduction or development of an effective vaccine against HAdV-55 and HAdV-4 should be considered.
Dr. Heo is a physician in the Department of Infectious Diseases at Ajou Unversity School of Medicine. His current research interests are the epidemiology of vaccine-preventable and vectorborne diseases.
Dr. Noh is a physician in the Division of Infectious Diseases at Korea University Guro Hospital. Her current research interests are respiratory viruses and emerging infectious diseases.
Acknowledgments
This work was supported by a grant from the Armed Forces Medical Command, South Korea.
References
- Hwang SM, Park DE, Yang YI, Park SJ, Lee HK, Kim MJ, et al. Outbreak of febrile respiratory illness caused by adenovirus at a South Korean military training facility: clinical and radiological characteristics of adenovirus pneumonia. Jpn J Infect Dis. 2013;66:359–65. DOIPubMed
- Sanchez JL, Cooper MJ, Myers CA, Cummings JF, Vest KG, Russell KL, et al. Respiratory infections in the U.S. military: recent experience and control. Clin Microbiol Rev. 2015;28:743–800. DOIPubMed
- Yoshitomi H, Sera N, Gonzalez G, Hanaoka N, Fujimoto T. First isolation of a new type of human adenovirus (genotype 79), species Human mastadenovirus B (B2) from sewage water in Japan.J Med Virol. 2017;89:1192–200. DOIPubMed
- Lin KH, Lin YC, Chen HL, Ke GM, Chiang CJ, Hwang KP, et al. A two decade survey of respiratory adenovirus in Taiwan: the reemergence of adenovirus types 7 and 4. J Med Virol. 2004;73:274–9. DOIPubMed
- Gray GC, McCarthy T, Lebeck MG, Schnurr DP, Russell KL, Kajon AE, et al. Genotype prevalence and risk factors for severe clinical adenovirus infection, United States 2004-2006. Clin Infect Dis. 2007;45:1120–31. DOIPubMed
- Lynch JP III, Kajon AE. Adenovirus: epidemiology, global spread of novel serotypes, and advances in treatment and prevention. Semin Respir Crit Care Med. 2016;37:586–602. DOIPubMed
- Gray GC, Callahan JD, Hawksworth AW, Fisher CA, Gaydos JC. Respiratory diseases among U.S. military personnel: countering emerging threats. Emerg Infect Dis. 1999;5:379–85. DOIPubMed
- Gaydos CA, Gaydos JC. Adenovirus vaccines in the U.S. military. Mil Med. 1995;160:300–4. DOIPubMed
- Radin JM, Hawksworth AW, Blair PJ, Faix DJ, Raman R, Russell KL, et al. Dramatic decline of respiratory illness among US military recruits after the renewed use of adenovirus vaccines. Clin Infect Dis. 2014;59:962–8. DOIPubMed
- Centers for Disease Control and Prevention (CDC). Acute respiratory disease associated with adenovirus serotype 14—four states, 2006-2007. MMWR Morb Mortal Wkly Rep. 2007;56:1181–4.PubMed
- Metzgar D, Osuna M, Kajon AE, Hawksworth AW, Irvine M, Russell KL. Abrupt emergence of diverse species B adenoviruses at US military recruit training centers. J Infect Dis. 2007;196:1465–73. DOIPubMed
- Heo JY, Lee JE, Kim HK, Choe KW. Acute lower respiratory tract infections in soldiers, South Korea, April 2011-March 2012. Emerg Infect Dis. 2014;20:875–7. DOIPubMed
- Kim SJ, Kim K, Park SB, Hong DJ, Jhun BW. Outcomes of early administration of cidofovir in non-immunocompromised patients with severe adenovirus pneumonia. PLoS One. 2015;10:e0122642. DOIPubMed
- Park JY, Kim BJ, Lee EJ, Park KS, Park HS, Jung SS, et al. Clinical features and courses of adenovirus pneumonia in healthy young adults during an outbreak among Korean military personnel.PLoS One. 2017;12:e0170592. DOIPubMed
- Chmielewicz B, Benzler J, Pauli G, Krause G, Bergmann F, Schweiger B. Respiratory disease caused by a species B2 adenovirus in a military camp in Turkey. J Med Virol. 2005;77:232–7. DOIPubMed
- Kajon AE, Dickson LM, Metzgar D, Houng HS, Lee V, Tan BH. Outbreak of febrile respiratory illness associated with adenovirus 11a infection in a Singapore military training cAMP. J Clin Microbiol. 2010;48:1438–41. DOIPubMed
- Walsh MP, Seto J, Jones MS, Chodosh J, Xu W, Seto D. Computational analysis identifies human adenovirus type 55 as a re-emergent acute respiratory disease pathogen. J Clin Microbiol. 2010;48:991–3. DOIPubMed
- Li X, Kong M, Su X, Zou M, Guo L, Dong X, et al. An outbreak of acute respiratory disease in China caused by human adenovirus type B55 in a physical training facility. Int J Infect Dis. 2014;28:117–22. DOIPubMed
- Casas I, Avellon A, Mosquera M, Jabado O, Echevarria JE, Campos RH, et al. Molecular identification of adenoviruses in clinical samples by analyzing a partial hexon genomic region. J Clin Microbiol. 2005;43:6176–82. DOIPubMed
- Tamura K, Stecher G, Peterson D, Filipski A, Kumar S. MEGA6: molecular evolutionary genetics analysis version 6.0. Mol Biol Evol. 2013;30:2725–9. DOIPubMed
- Zhu Z, Zhang Y, Xu S, Yu P, Tian X, Wang L, et al. Outbreak of acute respiratory disease in China caused by B2 species of adenovirus type 11. J Clin Microbiol. 2009;47:697–703. DOIPubMed
- Cao B, Huang GH, Pu ZH, Qu JX, Yu XM, Zhu Z, et al. Emergence of community-acquired adenovirus type 55 as a cause of community-onset pneumonia. Chest. 2014;145:79–86. DOIPubMed
- Lafolie J, Mirand A, Salmona M, Lautrette A, Archimbaud C, Brebion A, et al. Severe pneumonia associated with adenovirus type 55 infection, France, 2014. Emerg Infect Dis. 2016;22:2012–4. DOIPubMed
- Kim YJ, Hong JY, Lee HJ, Shin SH, Kim YK, Inada T, et al. Genome type analysis of adenovirus types 3 and 7 isolated during successive outbreaks of lower respiratory tract infections in children. J Clin Microbiol. 2003;41:4594–9. DOIPubMed
- Lee J, Choi EH, Lee HJ. Clinical severity of respiratory adenoviral infection by serotypes in Korean children over 17 consecutive years (1991-2007). J Clin Virol. 2010;49:115–20. DOIPubMed
- Yoo H, Gu SH, Jung J, Song DH, Yoon C, Hong DJ, et al. Febrile respiratory illness associated with human adenovirus type 55 in South Korea military, 2014–2016. Emerg Infect Dis. 2017;23:1016–20. DOIPubMed
- Barker JH, Luby JP, Sean Dalley A, Bartek WM, Burns DK, Erdman DD. Fatal type 3 adenoviral pneumonia in immunocompetent adult identical twins. Clin Infect Dis. 2003;37:e142–6. DOIPubMed
- Lewis PF, Schmidt MA, Lu X, Erdman DD, Campbell M, Thomas A, et al. A community-based outbreak of severe respiratory illness caused by human adenovirus serotype 14. J Infect Dis. 2009;199:1427–34. DOIPubMed
- Ludwig SL, Brundage JF, Kelley PW, Nang R, Towle C, Schnurr DP, et al. Prevalence of antibodies to adenovirus serotypes 4 and 7 among unimmunized US Army trainees: results of a retrospective nationwide seroprevalence survey. J Infect Dis. 1998;178:1776–8. DOIPubMed
- Sanchez JL, Binn LN, Innis BL, Reynolds RD, Lee T, Mitchell-Raymundo F, et al. Epidemic of adenovirus-induced respiratory illness among US military recruits: epidemiologic and immunologic risk factors in healthy, young adults. J Med Virol. 2001;65:710–8. DOIPubMed
- Trei JS, Johns NM, Garner JL, Noel LB, Ortman BV, Ensz KL, et al. Spread of adenovirus to geographically dispersed military installations, May-October 2007. Emerg Infect Dis. 2010;16:769–75. DOIPubMed
Figures
Tables
Suggested citation for this article: Heo JY, Noh JY, Jeong HW, Choe KW, Song JY, Kim WJ, et al. Molecular epidemiology of human adenovirus–associated febrile respiratory illness in soldiers, South Korea. Emerg Infect Dis. 2018 Jul [date cited]. https://doi.org/10.3201/eid2407.171222
1Preliminary results from this study were presented at the European Congress of Clinical Microbiology and Infectious Diseases 2015, convened April 25–28, 2015, in Copenhagen, Denmark.
2These authors contributed equally to this article.






















.png)










No hay comentarios:
Publicar un comentario