
Oncolytic Virus Therapy: Using Tumor-Targeting Viruses to Treat Cancer
February 9, 2018, by NCI Staff
For more than a century, doctors have been interested in using viruses to treat cancer, and in recent years a small but growing number of patients have begun to benefit from this approach.
Some viruses tend to infect and kill tumor cells. Known as oncolytic viruses, this group includes viruses found in nature as well as viruses modified in the laboratory to reproduce efficiently in cancer cells without harming healthy cells.
To date, only one oncolytic virus—a genetically modified form of a herpesvirus for treating melanoma—has been approved by the Food and Drug Administration (FDA), though a number of viruses are being evaluated as potential treatments for cancer in clinical trials.
Oncolytic viruses have long been viewed as tools for directly killing cancer cells. But a growing body of research suggests that some oncolytic viruses may work—at least in part—by triggering an immune response in the body against the cancer.
When a virus infects a tumor cell, the virus makes copies of itself until the cell bursts. The dying cancer cell releases materials, such as tumor antigens, that allow the cancer to be recognized, or “seen,” by the immune system.
“Oncolytic viruses are alerting the immune system that something’s wrong,” said Jason Chesney, M.D., Ph.D., director of the University of Louisville’s James Graham Brown Cancer Center. This can lead to an immune response against nearby tumor cells (a local response) or tumor cells in other parts of the body (a systemic response).
For this reason, some researchers consider oncolytic viruses to be a form of immunotherapy—a treatment that harnesses the immune system against cancer. But many in the field would agree that more studies are needed to learn how different oncolytic viruses work against cancer.
A Modern Approach to an Old Idea
Since the late 1800s, doctors have observed that some patients with cancer go into remission, if only temporarily, after a viral infection. Today, several dozen viruses—and a few strains of bacteria—are being studied as potential cancer treatments, according to research presented at an NCI-sponsored conference on using microbes as cancer therapies in 2017.
“Oncolytic virus therapy is of growing interest to researchers for one reason: It’s working,” said Juan Fueyo, M.D., of the University of Texas MD Anderson Cancer Center, who co-developed a type of oncolytic virus being tested in patients with brain tumors.
Although the notion of using viruses in cancer therapy is old, the science only began to move forward in the 1990s with advances in genetic engineering technology, noted Matthias Gromeier, M.D., of the Duke Cancer Institute, who has led clinical trials of a genetically modified form of poliovirus.
“There was another shift—around 2005—as people began to realize that the true value of viruses in cancer therapy is in immunotherapy,” Dr. Gromeier continued. “Today, viruses are firmly established as a potential option to enhance and mediate immunotherapy.”
He added: “These are still early days for oncolytic viruses, but it’s now getting interesting.”
The First FDA-Approved Oncolytic Virus Therapy
The first oncolytic virus to receive FDA approval was a treatment for melanoma known as talimogene laherparepvec (Imlygic®), or T-VEC. The treatment, which is injected into tumors, was engineered to produce a protein that stimulates the production of immune cells in the body and to reduce the risk of causing herpes.
In some patients receiving the therapy, tumors that could not be injected have shrunk, suggesting that T-VEC can generate a systemic immune response, noted Howard Kaufman, M.D., of the Rutgers Cancer Institute of New Jersey.
“The oncolytic virus kills tumor cells and causes the release of danger signals, which help to generate an immune response,” explained Dr. Kaufman, who co-led the clinical trial that led to the approval of T-VEC.
Investigating Interactions with the Immune System
At the NCI meeting about using microbes as cancer therapies last year, more than 350 investigators discussed many topics, including the need to better understand how infectious agents interact with tumors and with components of the immune system.
The biological mechanisms used by viruses to kill tumors depend on various factors, including the virus, the target tissue or cell, and which biological pathways are targeted, according to Phillip Daschner of NCI’s Division of Cancer Biology, who helped organize the NCI conference.
Some viruses work primarily by killing tumor cells, whereas others work by directing local or systemic immune responses, he explained. Nonetheless, “there was a consensus at the meeting that even for directly oncolytic therapies, there probably is an important immune component to the response,” he added.
Dr. Kaufman noted that T-VEC, when given alone or in combination with other therapies, generally has been well tolerated by patients in clinical trials.
“We continue to be impressed by the safety profile of these approaches,” he said. “The quality of life for many of these patients is barely affected by these agents.”
Using Viruses to Enhance the Body’s Immune Response
One of the challenges for researchers now is to try to enhance the immune response to the tumor through a variety of strategies, including by combining oncolytic virus therapy and immunotherapy.
The promise of this approach has been demonstrated in two early-phase clinical trials. Patients with melanoma who received T-VEC plus a type of immunotherapy known as a checkpoint inhibitor had higher response rates than those who received a checkpoint inhibitor alone.
In one trial, nearly 200 patients received T-VEC with or without ipilimumab (Yervoy®). The results suggested to the researchers that the combination therapy could induce an immune response. “To me, that’s the big finding of this study,” said Dr. Chesney, who co-led the clinical trial with Dr. Kaufman.
In the second trial, which included 21 patients, T-VEC was combined with pembrolizumab (Keytruda®). The oncolytic virus induced the infiltration of immune cells known as T cellsinto tumors that had low levels of these cells prior to treatment, the researchers found.
The study suggests that the viral therapy can change the local microenvironment to make an immunologically “cold” tumor—that is, a tumor lacking T cells—into an inflamed, or “hot,” tumor, noted John B.A.G. Haanen, Ph.D., of the Netherlands Cancer Institute in a commentary accompanying the study results.
“The injection [of T-VEC] is like lighting a match—it’s the spark that starts a fire,” said Antoni Ribas, M.D., Ph.D., of the UCLA Jonsson Comprehensive Cancer Center, who led the trial. The therapy was generally well tolerated, he noted, and the most common side effects were fatigue, fever, and chills.
A phase 3 clinical trial involving 600 patients with melanoma who will receive T-VEC with or without pembrolizumab is under way to assess the combination therapy in a large, randomized study.
The same combination—T-VEC plus pembrolizumab—is also being evaluated in a clinical trial for patients with advanced melanoma that has progressed despite treatment with a checkpoint inhibitor such as pembrolizumab or nivolumab (Opdivo®).
This NCI-sponsored trial is testing the idea that injections of T-VEC into accessible melanoma tumors will increase the infiltration of immune cells into these and potentially other tumors, making them susceptible to treatment with pembrolizumab.
A New Way of Delivering Viruses
Most oncolytic virus therapies have been tested in patients with melanoma or brain tumors, and most treatments have been given as injections into tumors. Two new studies highlight efforts to expand the number of cancer types treated with oncolytic virus therapies as well as the methods of delivery.
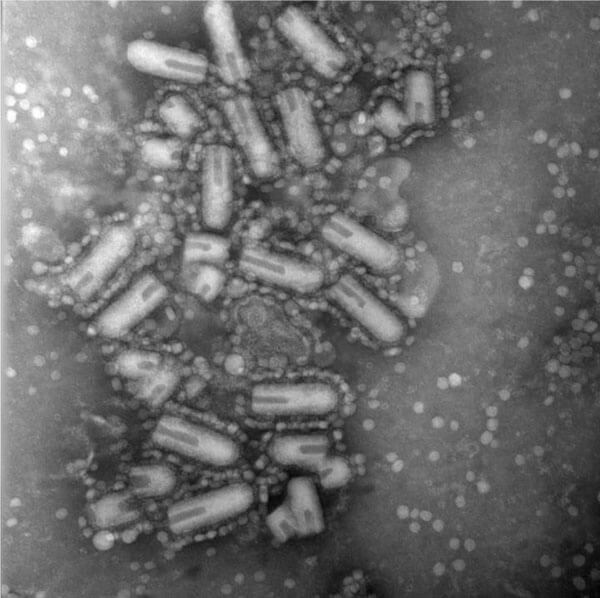
One of the studies found that an oncolytic virus delivered intravenously could cross the blood–brain barrier and enter brain tumors, killing tumor cells. The treatment uses a type of virus known as a reovirus, which causes mild symptoms of a cold or stomach bug in children.
In the second study, researchers tested the Maraba virus, which was originally isolated from a species of sand fly in Brazil, as a way to sensitize tumors to immunotherapy in a mouse model of triple-negative breast cancer.
In both studies, the researchers found that giving oncolytic virus therapy prior to surgery may alter the body’s immune response and enhance the effects of subsequent treatment with a checkpoint inhibitor.
“Combination immunotherapies like these may be most effective when used early in treatment when tumor burden is less and immune systems are intact,” noted Marie-Claude Bourgeois-Daigneault, Ph.D., of the University of Ottawa, an investigator on the Maraba virus study.
Testing a Modified Form of Poliovirus against Brain Tumors
At the Duke Cancer Institute, Dr. Gromeier and his colleagues have been testing an engineered poliovirus, called PVS-RIPO, in patients with glioblastoma.
When the research began in the mid-1990s, Dr. Gromeier viewed oncolytic viruses primarily as agents for killing cancer cells. His thinking changed, however, as PVS-RIPO was tested in patients, and his team noticed clinical changes associated with immune responses in the patients.
“From the first patients, we observed very clear signs that the virus elicited antitumor immune responses,” Dr. Gromeier recalled. Some patients had swelling in the brain and “profound changes in the tumor that took months to develop, which is consistent with an immune event,” he explained.
Based on the results of the clinical studies, FDA in 2016 granted “breakthrough status” to Duke’s poliovirus therapy, which allows officials at FDA to accelerate the agency’s review of the therapy for approval.
“We are interested in exploring what we can combine with PVS-RIPO,” said Dr. Gromeier. “Everyone seems to agree that no single mode of treatment will do the trick in treating cancer.”
A phase 2 trial testing PVS-RIPO with or without the chemotherapy drug lomustine (Gleostine®) is under way in patients with glioblastoma.
Investigating the Mechanisms of Oncolytic Virus Therapy
To learn more about the mechanisms by which poliovirus therapy attacks tumor cells, the Duke researchers recently conducted experiments in cancer cell lines and in mice.
They found that cancer cells infected with PVS-RIPO released tumor antigens and other material that activated immune cells called dendritic cells and induced an immune response against the cancer cells.
“In the mouse model, we showed that a poliovirus could induce a T-cell response that recognizes the tumor,” said Smita Nair, Ph.D., of the Duke University School of Medicine. The finding provides further support for testing the oncolytic virus in combination with other types of immunotherapies, including checkpoint inhibitors, she added.
The Duke team is planning a clinical trial to test PVS-RIPO in six patients with triple-negative breast cancer. Two weeks before undergoing surgery, the patients will receive injections of the treatment into their tumors and will be followed to determine whether the poliovirus triggers any changes in immune system molecules or in the tumor.
Future Research Questions and Priorities for the Field
As oncolytic viruses are tested in clinical trials, researchers will try to learn which patients are likely to respond. “We need biomarkers to help develop effective combination therapies and to select patients who are most likely to benefit from certain combinations,” said Dr. Nair.
Another challenge for the field will be to use the knowledge gained from the melanoma clinical trials to develop treatments for patients with other types of tumors, Dr. Chesney noted.
For researchers, it will also be important to understand “how much tumor infection and killing is required to treat cancer,” said Dr. Gromeier. “These are critical questions that we need to answer, and we’re working on it.”
Oncolytic Viruses May Also Reveal Insights into Immunotherapy
Research on oncolytic viruses may yield insights into the use of current immunotherapies.
“Viruses are great tools for helping us to understand how the antitumor immune response works,” said Dr. Fueyo of MD Anderson. “What we learn from viruses will help us move the field of immunotherapy forward.”
The evolution in thinking about oncolytic viruses since Dr. Fueyo began working in the field two decades ago represents an important shift that has implications for future research.
“We used to think only about making viruses better—more powerful—at killing tumor cells,” said Dr. Fueyo. “Now we need to find ways to help viruses enhance the immune response.”




















.png)












No hay comentarios:
Publicar un comentario