Focus: Scientists encourage holistic study of infectious and noncommunicable diseases
November / December 2019 | Volume 18, Number 6

Photo by Richard Lord for Fogarty/NIH
The growing convergence of infectious and noncommunicable
diseases requires a more integrated approach to research and
training, a recent NASEM report said.
diseases requires a more integrated approach to research and
training, a recent NASEM report said.
The research community has traditionally viewed diseases as either infectious or noncommunicable. With the growing evidence this is a false distinction, a group of scientists recently convened to examine the issue and have produced a report titled, Breaking Down Silos: the Convergence of Infectious Diseases and Noncommunicable Diseases (NCDs) .
The findings are based on discussions held during a workshop in July 2019 convened by the National Academies of Sciences, Engineering and Medicine (NASEM). The effort was supported by NASEM and other public and private partners, including NIH’s National Institute of Allergy and Infectious Diseases. A committee convened discussants from industry, academia, government, nongovernmental organizations and NASEM staff, and was chaired by Fogarty grantee Dr. Peter Daszak, president of the EcoHealth Alliance, one of the funding partners.
Breaking Down Silos: the
Convergence of Infectious Diseases
and Noncommunicable Diseases
National Academies of Sciences,
Engineering and Medicine (NASEM),
2019
While there’s a growing recognition of the links between infectious diseases and NCDs, “the two fields continue to be isolated from each other, with the two realms often supported by separate funding streams, studied using divergent research methodologies, and shaped by vertical health policies and programs,” the report noted. Yet scientists have known for decades, for instance, that Helicobacter pylori causes gastric inflammation, ulcers and gastritis.
More recent discoveries have found that human papillomavirus is linked to cervical cancer, and that hepatitis B and C can lead to chronic liver disease. Another example is Borrelia burgdorferi, which can cause Lyme disease.
The authors warn that epidemics of both infectious diseases and NCDs are expanding globally and are poised to affect huge numbers of people in the coming decades. NCDs disproportionately affect people in low- and middle-income countries (LMICs), where 32 million are dying from NCDs - nearly half before the age of 70 - according to the WHO.
A constellation of factors is spurring the merging of infectious diseases and NCDs, the report said. Globalization and environmental factors cause increased spread of pathogens, while urbanization and lifestyle changes contribute to the rise in NCDs. “The convergent dynamics among microbes, infections, NCDs, normal health functioning and shared risk factors are complex and intertwined,” the authors said.
Multiple morbidities involving both infectious diseases and NCDs add another layer of complexity. Recent discoveries regarding the human microbiome have illuminated its role in health and its relationship to diet, lifestyle and use of antibiotics. Dozens of NCDs have already been shown to be related to the microbiome.
“Research has only begun to reveal the enormous complexity of the microbial world and the extent to which microbes interact with humans and influence human health,” the report said. Gaining a better understanding of these linkages and bridging cross-sectoral collaborations would help advance research, develop better prevention and treatment interventions, and reduce the public health impact of both infectious disease and NCDs.
- Related report chapter: Chapter 1 Introduction - The Convergence of Infectious Diseases and Noncommunicable Diseases
Data show colliding epidemics
Shifting trends in global mortality warrant convergent action against the colliding epidemics of infectious diseases and NCDs, according to Dr. Tolullah Oni of the University of Cambridge. Oni presented 2015 data from the Disease Control Priorities project that showed only three of the top 10 contributors to the global crude death rate were infectious diseases. By contrast, NCDs represented seven of the top 10, with considerable increases in dementias, diabetes, lung cancer and heart disease. In low-income countries, respiratory infections were the largest cause of death, with stroke and heart disease ranking second and third.
Infectious diseases not only co-occur with NCDs but also interact with them, driving a rise in multi-morbidity, Oni explained. In South Africa, a national survey found double, triple and even quadruple multimorbidity. Significant numbers of people suffer from a combination of diabetes-hypertension-HIV or TB-diabetes-hypertension. Also common were those with hypertension-diabetes-TB-HIV. Such multimorbidities are being seen in people at increasingly younger ages.
Moving toward convergence will require dispelling myths and false dichotomies, Oni said. Before the global HIV epidemic, the chronic nature of illness was thought to be an exclusive feature of NCDs. When that infectious disease proved to also have chronic characteristics, it catalyzed a shift in thinking about how to care for its comorbidities. Among people receiving treatment for HIV, about 20% have another condition such as hypertension, TB or diabetes.
There’s also a false presumption that the causal relationship between NCDs and infectious diseases only works in one direction, Oni said. However, evidence suggests it is bidirectional. For instance, a 2015 study found the emergence of smoking and alcohol abuse are risk factors for TB, in addition to widely acknowledged causes such as HIV and malnutrition.
Many believe NCDs and infectious diseases have distinct risk factors. In fact, shared risk factors are a potential starting point for convergent action, Oni suggested. Rapid urbanization creates an additional layer of complexity that requires identifying shared risk factors and developing strategies to address them.
Unhealthy environments can impede healthy lifestyle choices, contributing to NCDs. In addition, infectious and zoonotic diseases are reemerging as rapid urbanization has pushed the boundaries of human settlements. Oni proposed broadening the concept of health services to include habitation planning, transportation, water and waste, and food - since all of these can affect both infectious disease and NCDs.
- Related report chapter: Chapter 2 An Overview of Colliding Epidemics and Syndemics
Gum disease may spur Alzheimer’s
There’s growing evidence to support a hypothesis that a brain infection could be a driver of Alzheimer’s disease, according to presenter Casey Lynch, CEO of Cortexyme, Inc. A decade ago, tooth loss, periodontal disease and the bacterium P. gingivalis were established as risk factors for Alzheimer’s, Lynch said. Studies have suggested that having gum disease in middle-age increased the risk for developing Alzheimer’s later in life.
While epidemiology cannot prove causation, Lynch said researchers wonder if P. gingivalis is entering the brain and contributing to dementia. Half of elderly people have periodontal disease and the vast majority are infected with this bacterium, Lynch reported. If a person flosses and has bleeding gums, the pathogen can enter the circulatory system and may enter the brain. In animal models, infection with P. gingivalis does infiltrate the brain and causes inflammation, which triggers development of amyloid plaques. Studies of a new drug in animals suggest treating the infection can potentially make damaged neurons function again.
Epstein-Barr virus causes NCDs
More than 95 percent of the world’s population is infected with the Epstein-Barr virus (EBV), according to panelist Dr. John Harley of Cincinnati’s Children’s Hospital Medical Center. Many NCDs are linked to EBV, including lupus, multiple sclerosis, rheumatoid arthritis and type 1 diabetes. By studying genetic markers for the diseases, scientists hope to discover how they are triggered.
NCDs can boost risk of infections
There are known and suspected risks that chronic diseases pose to the development and severity of infectious diseases, according to two experts who presented case studies.
Research has shown that having a high body mass index (BMI) is associated with increased risk for infections. Dr. Christopher Thaiss of the University of Pennsylvania said he and his team are studying mice to try to figure out why that is. His results suggest hyperglycemia causes an intestinal barrier problem that drives susceptibility to enteric infection, he said.
Studies have shown that people with diabetes have roughly double the risk of developing active TB, and poorer outcomes for those receiving TB treatment, according to Dr. Julia Critchley of St. George’s University of London. Given the world regions with the highest predicted increases in diabetes over the next few decades - sub-Saharan Africa and Southeast Asia - are also where TB is endemic, Critchley says the population impact could be large.
- Related report chapter: Chapter 4 Risks Posed by Chronic Diseases to the Development and Severity of Infectious Diseases
Microbiome holds clues

Image courtesy of the National Human Genomics Research
Institute (NHGRI)
Human gut microbes can not only affect the body in obvious ways such as inflammatory bowel disease, but also in surprising ways including food allergies, liver disease and cardiovascular disease, according to Dr. Rob Knight of the University of California, San Diego.
In the 20th century, rates of multiple sclerosis, Crohn’s disease, type 1 diabetes and asthma skyrocketed. All four have now been shown to be associated with the human microbiome, Knight said. The NIH’s Human Microbiome Project is coordinating DNA studies so scientists can better understand the complex relationship of microbes to infectious diseases, NCDs and normal physiological functioning.
- Related report chapter: Chapter 5 Microbial Dimension to Human Development and Well-Being
Leveraging HIV platforms, Kenya’s AMPATH provides model
The relatively well-resourced HIV programs could be leveraged to provide NCD services, according to presenter Dr. Miriam Rabkin of Columbia University. The expansion of HIV treatment and prevention services has been successful with the leadership of communities and ministries of health, and with support from the global community and donors. HIV and some NCDs also share the same challenges such as the need for continuity of care. The prevalence of NCDs and NCD risk factors among people living with HIV is as high, or higher, than the rest of their communities, Rabkin noted.
Another lesson from HIV scale-up is the need to be realistic and innovative in dealing with resource constraints, including engaging the private sector, faith-based organizations, and civil society, she said.
HIV platforms can successfully be expanded to include NCDs, with Kenya’s AMPATH program as an example, its director Dr. Sylvester Kimaiyo said in a presentation to the workshop. AMPATH - an acronym for Academic Model Providing Access to Health care - incorporates care, research and training. Formed in 2001 to attract support for HIV services from outside the country, AMPATH expanded its focus to include NCDs in 2008.
In addition to close relationships with county governments and the national health ministry, AMPATH has formed academic partnerships with Moi University and a consortium led by Indiana University (IU). Over the years, AMPATH has benefitted from support from USAID, CDC and NIH. For example, a Fogarty grant to IU helped establish AMPATH’s electronic medical record system, which increased efficiencies and enabled research activities. AMPATH’s integrated approach includes a number of projects that are providing screening and care for chronic conditions.
- Related report chapter: Chapter 7 Integrating Health Care Delivery Models and Interventions
HIV program functions are applicable to noncommunicable diseases (NCDs)
Key Elements of Chronic Care Delivery Systems Examples Common to HIV and NCD Programs Diagnosis and enrollment Identification of risk factors, early diagnosis, opportunistic case-finding, point-of-service diagnostics, standardized diagnostic protocols. Retention and adherence Appointment systems, defaulter tracking, patient counseling, expert patients, secure medication supply chains, pharmacy support. Multidisciplinary family-focused care A multidisciplinary team of health care providers and community members delivers care in partnership with the patient. Longitudinal monitoring Health information systems have standardized and easily retrievable data. Linkages and referrals Links within the health facility (to lab, pharmacy, others), between facilities, and between facility and community. Self-management An informed, motivated patient is an effective manager of his/her own health. Community linkages and partnerships Need functional partnerships between health facility-based providers and community-based groups that facilitate access to services across the care continuum. Sources: Rabkin presentation, June 12, 2019; ICAP, 2011.
Research training must be integrated
Convergence of infectious and chronic diseases is already a reality for Dr. K. Srinath Reddy, president of India’s Public Health Foundation. He told the committee that his organization aims to address the diversity of health challenges across the spectrum of diseases. But to operationalize transdisciplinary research, health education must change, he said. It needs to produce individuals who acquire a transdisciplinary understanding and the ability to collaborate, even while they are developing depth in one area of research that is necessary to qualify them to become leaders, he said.

Photo by David Snyder for Fogarty/NIH
Fogarty grantee Dr. Patty Garcia - professor at Peru’s Cayetano
Heredia University - said research training programs should be
reconsidered to account for the convergence of infectious
and chronic diseases.
Heredia University - said research training programs should be
reconsidered to account for the convergence of infectious
and chronic diseases.
If dedicated funding streams could be established to bring together postdocs from different disciplines to work on multidisciplinary research challenges, Reddy said it could help build researchers who believe in the concept right from the beginning.
“We need to undo all the things that we have been doing for years,” suggested Dr. Patty Garcia, longtime Fogarty grantee and professor at Peru’s Cayetano Heredia University. The process should begin with rethinking training programs because the current system has created silos and overspecialization. The health education system should be more comprehensive and person-centered, she said.
The first priority should be to continue supporting research on the convergence of infectious and chronic diseases that takes into consideration life course, gender, ethnicity and diverse environments, Garcia said. Secondly, a shift in thinking is needed to bring research into policies for prevention, surveillance and detection, control and treatment, she said. While funders tend to prefer randomized controlled trials (RCTs), qualitative research and descriptive epidemiology within conceptual models should be prioritized as well. Since RCTs are carried out in sterile settings, the research output usually fails to become policy because the reality is more complex than the research environment, she said. Systems-based research can be leveraged across sectors and provide cost-effectiveness analyses and other information that is useful for policymakers.
- Related report chapter: Chapter 9 Visionary Statements on Potential Priorities to Address the Convergence
NCD advocacy needed to improve equity
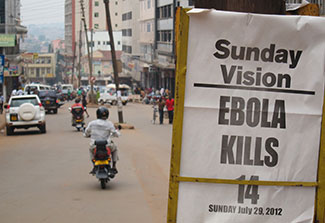
Photo courtesy of CDC
Competition with the urgency of infectious disease pandemics
makes it hard to convince policymakers that it’s also important
to invest in NCDs, the study said.
makes it hard to convince policymakers that it’s also important
to invest in NCDs, the study said.
Disease convergence presents a complex, tangled web of information and ideas, said Daszak in his closing remarks. The community should try to grasp nuggets of value that could be used to communicate effectively with policymakers, he suggested.
Many people working on infectious diseases and NCDs may be self-selecting their respective silos, which are reinforced through different belief systems and behaviors, separate journals, distinct funding streams and disparate research methods, Daszak observed. That may make it more difficult to break down the silos.
Finally, Daszak said the key lesson is that there is a massive inequity problem, yet convincing policymakers and politicians to invest in NCDs is enormously challenging, especially in competition with the urgency and concern surrounding infectious disease pandemics.
More Information
- The Convergence of Infectious Diseases and Noncommunicable Diseases: Proceedings of a Workshop (2019)
National Academies of Sciences, Engineering and Medicine (NASEM), 2019
To view Adobe PDF files, download current, free accessible plug-ins from Adobe's website .























.png)










No hay comentarios:
Publicar un comentario