Volume 25, Number 6—June 2019
Research Letter
Rickettsia japonica Infection after Land Leech Bite, Japan
On This Page
Figures
Downloads
Article Metrics
Eiichiro Sando , Motoi Suzuki, Mitsuya Katayama, Masakatsu Taira, Hiromi Fujita, and Koya Ariyoshi
, Motoi Suzuki, Mitsuya Katayama, Masakatsu Taira, Hiromi Fujita, and Koya Ariyoshi
Abstract
We report a case of Rickettsia japonica infection in an 81-year-old man in central Japan. The patient had fever, rash, and an eschar but no evidence of a tick bite. His symptoms began 8 days after a land leech bite. The land leech is a potential vector of R. japonica.
Japanese spotted fever, a tickborne disease caused by Rickettsia japonica, has been reported in Japan, Korea, and China (1–3). We describe a case of Japanese spotted fever after a land leech (Haemadipsa zeylanica japonica) bite.
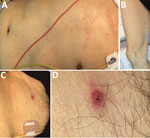
Figure. Patient with Rickettsia japonicainfection after being bitten by a land leech, Japan. A, B) Erythematous macular rash on the patient’s torso (A) and extremities (B); C, D) eschar on the...
On August 3, 2016, an 81-year-old man was transported to an emergency department with a 2-day history of fever (temperature of 38°C), staggering, appetite loss, and general malaise. He was undergoing hormonal therapy for prostate cancer and had an indwelling urinary catheter. However, he was fully independent and walked 2 km every day as a tour guide to a mountain road in the southern Boso area of Japan. At admission, he was alert and oriented, with no apparent fever (temperature of 36.8°C). Clinicians observed a nonpruritic, painless rash on his torso and extremities (Figure, panels A, B), including his palms and the soles of his feet. The attending physician thoroughly searched for an eschar and noted only a single nonpruritic, painless lesion on the man’s lower abdomen (Figure, panel C). The patient and his family reported that the eschar appeared at the site where a land leech had been attached on July 24, 10 days before admission, and that the site bled when the leech was removed. They denied any tick bite.
Notable laboratory data included low platelet count (102,000/µL), slightly elevated aspartate aminotransferase (52 IU/L), elevated lactate dehydrogenase (468 IU/L), and elevated C-reactive protein (5.37 mg/dL). Urinalysis was positive for protein and occult blood. Chest radiograph and electrocardiogram findings were unremarkable.






















.png)










No hay comentarios:
Publicar un comentario