Volume 20, Number 7—July 2014
Research
Borrelia miyamotoi sensu lato Seroreactivity and Seroprevalence in the Northeastern United States
Downloads
Altmetric
63
of this article EID Journal Metrics on
Peter J. Krause , Sukanya Narasimhan, Gary P. Wormser, Alan G. Barbour, Alexander E. Platonov, Janna Brancato, Timothy Lepore, Kenneth Dardick, Mark Mamula, Lindsay Rollend, Tanner K. Steeves, Maria Diuk-Wasser, Sahar Usmani-Brown, Phillip Williamson, Denis S. Sarksyan, Erol Fikrig, Durland Fish, and the Tick Borne Diseases Group
, Sukanya Narasimhan, Gary P. Wormser, Alan G. Barbour, Alexander E. Platonov, Janna Brancato, Timothy Lepore, Kenneth Dardick, Mark Mamula, Lindsay Rollend, Tanner K. Steeves, Maria Diuk-Wasser, Sahar Usmani-Brown, Phillip Williamson, Denis S. Sarksyan, Erol Fikrig, Durland Fish, and the Tick Borne Diseases Group
Abstract
Borrelia miyamotoi sensu lato, a relapsing fever Borrelia sp., is transmitted by the same ticks that transmit B. burgdorferi (the Lyme disease pathogen) and occurs in all Lyme disease–endemic areas of the United States. To determine the seroprevalence of IgG against B. miyamotoi sensu lato in the northeastern United States and assess whether serum from B. miyamotoi sensu lato–infected persons is reactive to B. burgdorferi antigens, we tested archived serum samples from area residents during 1991–2012. Of 639 samples from healthy persons, 25 were positive for B. miyamotoi sensu lato and 60 for B. burgdorferi. Samples from ≈10% of B. miyamotoi sensu lato–seropositive persons without a recent history of Lyme disease were seropositive for B. burgdorferi. Our resultsA suggest thatA human B. miyamotoiA sensu latoA infection may be common in southern New England and that B. burgdorferiantibody testing is not an effective surrogate for detecting B. miyamotoi sensu lato infection.
Relapsing fever, an arthropod-borne infection caused by several Borrelia spp. spirochetes, is transmitted by ticks and lice (1,2). In 1995, Fukunaga et al. (3) discovered a novel relapsing fever spirochete in the hard-bodied (ixodid) tick Ixodes persulcatus and named it Borrelia miyamotoi. This discovery greatly expanded the potential geographic range of relapsing fever borreliae for humans. Before this finding, only soft-bodied ticks were known to transmit tick-borne relapsing fever spirochetes to humans. In 2001, a related spirochete was detected in I. scapularis ticks in the northeastern United States (4); this and similar organisms have been designated B. miyamotoi sensu lato to distinguish them from the B. miyamotoi sensu stricto isolates from Japan (5). A subsequent study showed that ticks in 15 states in the northeastern and northern midwestern regions of the United States are infected with B. miyamotoi sensu lato and have an average prevalence of infection of 1.9% (range 0–10.5%) (6). B. miyamotoi sensu lato has now been found in all tick species known to be vectors of Lyme disease, including I. pacificus in the western United States, I. ricinus in Europe, and I. persulcatus and I. ricinus in Russia (7–9). The first human cases of B. miyamotoi sensu lato infection were reported from central Russia in 2011 (9). Several reports of B. miyamotoi sensu lato infection in humans have subsequently been published, including 3 in the United States, 1 in Europe, and 1 in Russia (10–14). Some of these reports suggest that B. miyamotoi sensu lato infection causes a nonspecific, virus-like illness. B. miyamotoi sensu lato and B. burgdorferi, the agent of Lyme disease, share several antigens that might cause cross-reactivity during serologic testing, which could lead to a misdiagnosis.
There are few data on the seroprevalence of B. miyamotoi sensu lato infection. To increase knowledge of the seroprevalence of this infection, we used assays for antibodies against B. miyamotoi sensu lato glycerophosphodiester phosphodiesterase (GlpQ), a protein that is absent from all Lyme disease Borreliaspecies (15), for evaluation of >1,000 archived serum samples from persons living in a Lyme disease–endemic region of the United States. We also performed standard 2-tiered testing for B. burgdorferi antibodies (16). Our aim was to compare the seroprevalence of B. miyamotoisensu lato with that of B. burgdorferi. We also sought to determine whether persons seropositive for B. miyamotoi sensu lato would also have positive results for standard B. burgdorferi antibody testing.
Study Population
The serum samples evaluated in our study were obtained during 1991–2012 from 3 groups of persons living in areas of the northeastern United States where Lyme disease is endemic. Group 1 consisted of 639 persons from Block Island and Prudence Island, Rhode Island, and from Brimfield, Massachusetts, who participated in serosurveys for tick-borne infections. Persons participating in the serosurvey were healthy at the time of blood sampling and were enrolled during the spring and autumn of each year (16). All participants were asked to respond to a questionnaire and to provide a blood sample for serologic analyses of tick-borne infections.
Group 2 consisted of 194 patients from Block Island; Nantucket, Massachusetts; Mansfield, Connecticut; and the Lower Hudson Valley, New York, who were enrolled in studies of tick-borne diseases. At or near the time of sample collection, persons in this group were treated with doxycycline, amoxicillin, or amoxicillin/clavulanic acid for acute Lyme disease.
Group 3 consisted of 221 adult patients who experienced a febrile illness in the late spring or summer without features suggestive of an upper respiratory tract infection or gastroenteritis. A subgroup of group 3 consisted of 17 patients from the Lower Hudson Valley who were enrolled in a study during 1992–2009 to better characterize the clinical and laboratory features of human granulocytic anaplasmosis as a single infection or as a co-infection with early Lyme disease. Results for serologic testing, culture, buffy coat examination for morulae, and/or PCR showed that none of the patients was infected with Anaplasma phagocytophilum (17). All these patients resided in an area where I. scapularis–transmitted infection is highly endemic and, thus, had possible exposure to I. scapularis ticks. A second subgroup of group 3 consisted of 204 adult patients from Block Island, Mansfield, or Nantucket who had suspected Lyme disease or babesiosis. Testing showed that 25 of these patients had babesiosis but none had Lyme disease or anaplasmosis.
Serum samples were also obtained from 2 patients from the Udmurtia Republic, Russia, who had PCR-confirmed acute B. miyamotoi sensu lato infection. In addition, Creative Testing Solutions (Tempe, AZ, USA) provided an aliquot of residual serum used for blood screening from 300 blood donors who lived in Tempe or in Miami, Florida.
De-identified serum samples were used in this study. The study was approved by the Yale School of Public Health Human Investigation Committee, the New York Medical College Institutional Review Board, and the University of Connecticut Institutional Review Board.
Laboratory Procedures
Production of B. miyamotoi sensu lato GlpQ Antigen
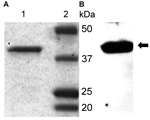
Figure 1. Polyacrylamide gel electrophoresis purification (A) and Western blot analysis (B) of recombinant glycerophosphodiester phosphodiesterase (rGlpQ)A) Coomassie blue staining of purified Borrelia miyamotoi sensu lato rGlpQ (lane 1) and of Precision Plus...
B. miyamotoi sensu lato glpQ from strain LB-2001 cloned into the prokaryotic expression vector pXT7 (18), a derivative of pGEM4Z and pSP64T (Promega, Madison, WI, USA), was transformed into BL21 Star (DE3)/pLysS cells (Invitrogen, Carlsbad, CA, USA), and transformants were used for protein production (6). The chromosome sequence for the protein is in GenBank (accession no. CP006647) (19). The 39.1-kDa recombinant GlpQ (rGlpQ) containing an N-terminal His tag was purified over an Ni-NTA Superflow affinity column (QIAGEN, Valencia, CA, USA) as described by the manufacturer. Purity was assessed by sodium dodecyl sulfate electrophoresis of ≈1 I1/4g of rGlpQ on a 4%–20% polyacrylamide gel and by Coomassie blue staining (Figure 1).
GlpQ Antibody ELISA
We developed a B. miyamotoi sensu lato IgG ELISA by using 20 C3H/HeJ mice (Jackson Laboratory, Bar Harbor, ME, USA). Ten of the mice were not infected. The other 10 age-matched mice were infected by using B. miyamotoi sensu lato–infected I. scapularis nymphal ticks. A month after the mice were infected, blood was obtained from all 20 mice for testing. Titrating concentrations of GlpQ protein and secondary antibody were tested in a checkerboard assay to determine the optimal concentrations for detecting B. miyamotoi sensu lato antibody. Results for the B. miyamotoi sensu lato ELISA were positive for all 10 B. miyamotoi sensu lato–infected mice and negative for all 10 uninfected mice.
To test the human serum samples, we coated ELISA plates with 100 I1/4L of 1 I1/4g/mL GlpQ protein in phosphate-buffered saline (PBS) and incubated the plates at 4° for 18 h. We then added 300 I1/4L of 1% bovine serum albumin in PBS buffer to the plates and incubated them for 2 h at room temperature. The plates were then emptied, and serum was added at a 1:320 dilution and incubated for 1 h. If acute- and convalescent-phase serum samples were available for a study participant, the initial dilution of the acute-phase sample was 1:80, and convalescent-phase samples were diluted to endpoint. The plates were then washed 3 times with wash buffer, and 100 I1/4L of goat antihuman IgG secondary antibody was added at 0.002 mg/mL, incubated for 1 h, and then washed 3 times. BluPhos substrate (Kirkegaard & Perry, Gaithersburg, MD, USA) was added and allowed to react for 20 min before absorbance at 630 nm was determined. B. miyamotoisensu lato–infected mouse serum was used as a positive control. As a negative control for each plate, we used serum samples that were negative for B. miyamotoi sensu lato antibody, as determined by ELISA and Western blot. The serum was obtained from 3 healthy participants who had no history of tick bite or tick-borne disease and who lived in an area where Lyme disease is endemic. The serum samples were tested by PCR for amplifiable B. miyamotoi sensu lato DNA and were negative. For mouse and human serum samples, a signal >3 SD above the mean of 3 noninfected serum controls was considered positive for B. miyamotoi sensu lato infection.
GlpQ Western Blot Antibody Assay
Purified GlpQ (500 ng) was electrophoresed on each replicate lane of a precast mini 4%–20% sodium dodecyl sulfate–polyacrylamide gel electrophoresis gel (Bio-Rad Laboratories, Hercules, CA, USA) and transferred to a nitrocellulose membrane using the Bio-Rad MiniTrans Blot Cell (Bio-Rad Laboratories). Replicate strips containing rGlpQ were blocked overnight at 4° in PBS (pH 7.2)/5% dried milk/0.05% Tween 20. The blocked strips were then individually incubated with human serum at a 1:250 dilution at room temperature in PBS (pH 7.2)/2.5% dried milk/0.05% Tween 20 for 1 h. The strips were then washed 3 times and incubated for 1 h with horseradish peroxidase–conjugated rabbit anti-human IgG (Sigma-Aldrich, St. Louis, MO, USA) or with horseradish peroxidase–conjugated goat anti-human IgM (Invitrogen) at a 1:5,000 dilution in PBS (pH 7.2)/2.5% dried milk/0.05% Tween 20. Bound antibodies were detected by using Thermo Scientific SuperSignal West Pico Chemiluminescent Substrate (Thermo Fisher Scientific, Inc., Rockford, IL, USA). Serum from ≈10% of the study participants reacted to a ≈55-kDa band, presumably a trace contaminant copurified with the rGlpQ generated in a bacterial expression system. Samples with a 39-kDa band corresponding to GlpQ on positive control mouse serum samples were considered GlpQ antibody–positive (Figure 1).
PCR DNA Amplification
B. burgdorferi Antibody Detection
We detected serologic evidence of exposure to B. burgdorferi by using a whole-cell sonicate ELISA, C6 ELISA, or Western blot assay as described (16,20–22). Specimens were considered positive according to the criteria of the US Centers for Disease Control and Prevention (http://www.cdc.gov/lyme/diagnosistesting/LabTest/TwoStep/index.html).
Case Definitions
B. miyamotoi sensu lato–seropositive serum samples were defined by the presence of B. miyamotoi sensu lato antibody as determined by using ELISA and confirmatory Western blot assays for IgG alone or IgG plus IgM antibody. B. burgdorferi seropositive serum samples were defined by the presence of B. burgdorferi antibody as determined by ELISA and supplemental Western blot IgM or IgG assays.
Study participants were considered to have B. miyamotoi sensu lato infection if they had exhibited a fever >37.5° and a >4-fold rise in antibody to B. miyamotoi sensu lato GlpQ protein between acute- and convalescent-phase serum samples, as determined by ELISA and confirmatory Western blot assays for IgG alone or IgG plus IgM. The time between acute- and convalescent-phase samples ranged from 2 wk to 2 mo. Study participants were considered to have Lyme disease if they had a physician-diagnosed erythema migrans skin lesion or a virus-like illness plus a test result that showed either PCR amplification of B. burgdorferi DNA in blood or B. burgdorferi seroconversion from negative to positive between acute- and convalescent-phase serum samples.
Statistical Analysis
A 2-tailed Fisher exact test was used to compare the frequency of B. miyamotoi sensu lato–seropositive and –seronegative study participants in groups 1, 2, and 3. The McNemar χ2 test was used to compare the seroprevalence of B. miyamotoi sensu lato and B. burgdorferi among group 1 participants.
Seroprevalence of B. miyamotoi sensu lato Infection
Serum samples from 52 of the 1,054 study participants were seroreactive to B. miyamotoi sensu lato antigen by rGlpQ ELISA and Western blot assay (Table 1). The percentage of B. miyamotoi sensu lato–seropositive persons was greater among participants with Lyme disease (group 2; 19/194 [9.8%]) than among those who were healthy (group 1; 25/639 [3.9%], p<0.01 by Fisher exact test, odds ratio [OR] 2.66 [range 1.35–5.16]) or those who had a febrile illness in the late spring or summer (group 3; 8/221 [3.6%], p<0.05 by Fisher exact test, OR 2.89 [range 1.17–7.81]). B. miyamotoi sensu lato DNA could not be amplified from any serum samples (including 27 acute-phase serum samples) from the 52 participants who had test results positive for B. miyamotoi sensu lato antibody.
Of the 639 serum samples from group 1 participants, 25 (3.9%) were seroreactive to B. miyamotoi sensu lato antigen and 60 (9.4%) were seroreactive to B. burgdorferi antigen, as determined by using the standard 2-step ELISA and Western blot procedure (McNemar χ2 test, p<0.0001, OR 10.23 [range 7.84–13.57]). About half (51%) of group 1 participants were male, and the mean age of group 1 participants was 55 years (range 2–102). There was no significant difference in the sex of the group 1 study participants who were seropositive for B. miyamotoi sensu lato (40% male) and those who were seropositive for B. burgdorferi (53% male; p = 0.34). The mean age also did not differ significantly between participants who were seropositive for B. miyamotoi sensu lato (59 years [+15]) and those who were seropositive for B. burgdorferi (61 years [+15]; p = 0.62).
Of the participants from Brimfield, Massachusetts, 9.3% (10/107) were seropositive for B. miyamotoi sensu lato and 7.5% (8/107) were seropositive for B. burgdorferi, compared with 3.2% (15/474) and 11% (52/474), respectively, of the participants from Block Island, Rhode Island. None of the 58 participants from Prudence Island, Rhode Island, were seropositive for B. miyamotoi sensu lato or B. burgdorferi.
Serodiagnosis of B. miyamotoi sensu lato Infection
To assess B. miyamotoi sensu lato ELISA and Western blot assay accuracy in patients with confirmed B. miyamotoi infection, we tested acute- and convalescent-phase serum samples from 2 patients in Russia with B. miyamotoi sensu lato infection confirmed by real-time PCR–(9). Both patients had a >4-fold rise in B. miyamotoi sensu lato GlpQ antibody between acute- and convalescent-phase serum samples (1:80 and 1:2,560, respectively, for 1 patient and 1:640 and 1:2,560, respectively, for the other), as determined by ELISA and confirmed by Western blot.
To assess B. miyamotoi sensu lato ELISA and Western blot assay performance in persons at low risk for Lyme disease or B. miyamotoi sensu lato infection, we performed the GlpQ ELISA on 300 serum samples from healthy blood donors living in Tempe or Miami. For the 9 microtiter plates used for this serosurvey, the mean and standard deviation of the ELISA optical density values for 3 negative control serum samples ranged from 0.108 to 0.136 and from 0.03 to 0.07, respectively. Of the 300 samples, 19 (6.3%) exceeded the mean of the negative control serum by >3 SDs, but none was reactive by Western blot.
We determined whether B. miyamotoi sensu lato infection might be misdiagnosed as Lyme disease in persons whose serum was reactive by B. burgdorferi antibody testing. Of the 36 B. miyamotoi sensu lato–seropositive study participants without a clinical history of Lyme disease within the previous 2 years, 7 (19.4%) had test results positive for B. burgdorferi by IgG and/or IgM ELISA, 6 (16.7%) had test results positive for C6 ELISA, and 4 (11.1%) had test results positive for standard 2-tier ELISA plus confirmatory Western blot (Table 2). The 2-tier B. burgdorferi ELISA and Western blot assay combination used in our laboratory has a 2% false-positive rate.
Clinical Manifestations among Patients with B. miyamotoi sensu lato Seroconversion

Figure 2. Western blot reactivity to recombinant Borrelia miyamotoiglycerophosphodiester phosphodiesterase in serum samples from 5 Borrelia miyamotoi sensu lato–seropositive patients in the northeastern United States, 1991–2012Numbers at the top of rows are...
A clinical description of illness was available for 5 symptomatic patients who experienced a ≥4 fold rise in B. miyamotoi sensu lato IgG and/or IgM antibody between acute- and convalescent-phase serum samples, as determined by ELISA and confirmatory Western blot assays (Western blot data shown in Figure 2). Of the 5 patients, 4 were co-infected with Lyme disease, 1 of whom was also co-infected with babesiosis (determined by blood smear). The 4 patients all had an erythema migrans skin lesion, and 2 had culture results positive for B. burgdorferi. The fifth patient had no evidence of co-infection and was the only 1 of 17 (5.9%) participants with a febrile summertime illness who had acute- and convalescent-phase serum tested for B. miyamotoi sensu lato antibody and who seroconverted. Three of these 5 patients have been reported previously (11). All 5 patients had fever, but a relapsing fever pattern was not reported. Symptoms resolved in 4 of the patients after treatment with doxycycline for 7–14 days, and symptoms resolved in the fifth patient after treatment with amoxicillin/clavulanic acid for 14 days.
We found evidence of human infection with the spirochete B. miyamotoi sensu lato in 52 residents residing in southern New England or New York State during 1991–2012. Among healthy study participants from southern New England, the seroprevalence of B. miyamotoisensu lato infection was about one third that of B. burgdorferi infection (3.9% vs. 9.4%, respectively). This finding is consistent with the higher rate of B. burgdorferi infection in I. scapularis ticks in the region (range 2:1–20:1) (4–6). As expected, the seroprevalence of B. miyamotoi sensu lato infection was higher in serum samples from patients with acute Lyme disease and recent I. scapularis tick bites than in serum samples from patients whose tick-bite status was unclear. B. miyamotoi sensu lato seroprevalence rates were similar among study participants with a febrile late spring or summertime illness and healthy participants, probably because B. miyamotoi sensu lato infection is unlikely to be a common cause of nonspecific febrile illness in the late spring or summer. The seroprevalence of B. miyamotoi sensu lato was less than that of B. burgdorferi but similar to that of Babesia microti among residents of the same southern New England and New York region (16,26–28).
Approximately 10 percent of the B. miyamotoi sensu lato–seropositive patients without a recent history of Lyme disease reacted to B. burgdorferi antigen by 2-tier testing. The reactivity could have represented a prior B. burgdorferi infection, a false-positive test reaction, and/or cross-reactivity of B. miyamotoi sensu lato antibody against >1 B. burgdorferi antigens. The frequency of antibody reactivity to B. burgdorferi in patients with relapsing fever is shown in Table 2 (23–25,29). Several proteins are found in common between B. burgdorferiand B. miyamotoi sensu lato, including the flagellin FlaB protein, the GroEL heat shock proteins, and the BmpA (P39) protein (19,25). Misdiagnosis of B. miyamotoi sensu lato infection as Lyme disease is therefore possible. Results of B. burgdorferi testing may be positive for B. miyamotoi sensu lato–infected patients who are co-infected with B. burgdorferi (as was the case for some persons in this study). Our findings suggest, however, that testing for antibodies against B. burgdorferi is not an appropriate surrogate for testing for antibodies against B. miyamotoi sensu lato; B. burgdorferi antibody testing should not be used in place of an assay for antibody against B. miyamotoisensu lato GlpQ or another B. miyamotoi sensu lato–specific antigen.
Our study had several limitations. First, laboratory evidence for acute B. miyamotoi sensu lato infection was based on ELISA and Western blot antibody assay rather than on culture, blood smear, or B. miyamotoi sensu lato PCR. However, in agreement with the case definition commonly used for many infectious diseases by the US Centers for Disease Control and Prevention (30), we considered results positive if a >4-fold rise in antibody occurred between acute- and convalescent-phase serum samples.
Second, B. miyamotoi sensu lato from North American has not been cultured, and blood smears were not available from the patients in our study. We were unable to detect B. miyamotoi sensu lato DNA in frozen, archived serum samples; however, the process of preparing serum from whole blood likely removed some spirochetes from the samples, and freeze–thaw cycles may have destroyed bacterial DNA. Furthermore, almost half of the serum samples that we tested were obtained after the period of acute illness, when the bacteremia may have cleared.
Third, our seroprevalence rates presumably would have been higher if we had tested for both IgM and IgG antibody by ELISA and included patients with IgM antibody alone as seropositive patients; however, we chose a more stringent definition of seropositivity by requiring the presence of IgG antibody. On the other hand, our seroprevalence data may have been inflated as a result of cross-reactivity of antibodies from other infections reacting against B. miyamotoi sensu lato GlpQ antigen. Although all other relapsing fever species have the glpQ gene, no other relapsing fever Borrelia sp. has been identified in I. scapularis ticks or humans in the northeastern United States (2,4–6,15,17,31).
Last, we do not have travel histories for the B. miyamotoi sensu lato–seroreactive patients included in the study, but the probability that many of our patients would have had exposure to other relapsing fever Borrelia spp. in the United States seems highly unlikely because these infections are infrequent and occur in the western states (2). Cross-reactivity against other tick-borne infections in the Northeast also appears unlikely because the agents of Lyme disease, human granulocytic anaplasmosis, and Powassan virus disease lack a glpQ gene (15). Proteins homologous to the GlpQ protein of relapsing fever borreliae are found in some gram-negative bacteria, including Escherichia coli, but they are so distant in sequence that antibody cross-reactivity is not expected (15).
The determination of B. miyamotoi sensu lato seroprevalence in our population is important because it indicates that this pathogen may infect persons at a rate that is similar to that of B. microti in the northeastern United States (16,23,24). Our data suggest that acute B. miyamotoi sensu lato infection in some persons may be misdiagnosed as Lyme disease because of the presence of antibody to B. burgdorferi from a previous B. burgdorferi infection, a false-positive test reaction, and/or cross-reactivity. Antibody testing for B. burgdorferi, however, is not adequate to detect infection with B. miyamotoi sensu lato in the United States. The potential for misdiagnosis may be greater in locations like northern California, were the prevalence of B. miyamotoi sensu lato in ticks equals or exceeds the prevalence of B. burgdorferi in ticks (32). Further studies are needed to better characterize the epidemiology and improve the serodiagnosis of human B. miyamotoi sensu lato infection.
Dr Krause is a Senior Research Scientist in the Department of Epidemiology of Microbial Diseases at the Yale School of Public Health and the Yale School of Medicine. His research focuses on tick-borne diseases, especially those caused by Borrelia miyamotoi and Babesia microti.
Acknowledgments
Members of the Tick Borne Diseases Group: Michel Ledizet and Mary Lou Breitenstein (L2 Diagnostics, LLC, New Haven, Connecticut, USA); Thomas Clay and Kathleen Stanton (Brimfield Family Health Center, Brimfield, Massachusetts, USA); Joseph Gadbaw (Lawrence and Memorial Hospital, New London, Connecticut); Janice Miller (Island Medical Center, Block Island, Rhode Island, USA); Ludmila S. Karan (Central Research Institute of Epidemiology, Moscow, Russia); and Kristen Brao (Yale School of Public Health, New Haven).
We thank Francesica Tizard at the Yale School of Public Health for help with manuscript preparation.
This work was supported by grants (AI088079 to D.F. and P.J.K. and AI100236 to A.G.B.) from the National Institute of Allergy and Infectious Diseases, National Institutes of Health. Additional support was provided by the Gordon and Llura Gund Foundation and the G. Harold and Leila Y. Mathers Charitable Foundation.
References
- Barbour AG. Relapsing fever. In: Goodman JL, Dennis DT, Sonenshine DE, editors. Tick-borne diseases of humans. Washington (DC): ASM Press; 2005.
- Dworkin MS, Schwan TG, Anderson DE. Tick-borne relapsing fever in North America. Med Clin North Am. 2002;86:417–33 .
- Fukunaga M, Takahashi Y, Tsuruta Y, Matsushita O, Ralph D, McClelland M, Genetic and phenotypic analysis of Borrelia miyamotoisp. nov., isolated from the ixodid tick Ixodes persulcatus, the vector for Lyme disease in Japan. Int J Syst Bacteriol. 1995;45:804–10 .
- Scoles GA, Papero M, Beati L, Fish D. A relapsing fever group spirochete transmitted by Ixodes scapularis ticks. Vector Borne Zoonotic Dis. 2001;1:21–34 .
- Bunikis J, Tsao J, Garpmo U, Berglund J, Fish D, Barbour AG. Typing of Borrelia relapsing fever group strains. Emerg Infect Dis. 2004;10:1661–4 .
- Barbour AG, Bunikis J, Travinsky B, Hoen AG, Diuk-Wasser MA, Fish D, Niche partitioning of Borrelia burgdorferi and Borrelia miyamotoi in the same tick vector and mammalian reservoir species. Am J Trop Med Hyg. 2009;81:1120–31.
- Mun J, Eisen RJ, Eisen L, Lane RS. Detection of a Borrelia miyamotoi sensu lato relapsing-fever group spirochete from Ixodes pacificusin California. J Med Entomol. 2006;43:120–3 .
- Richter D, Schlee DB, Matuschka FR. Relapsing fever–like spirochetes infecting European vector tick of Lyme disease agent. Emerg Infect Dis. 2003;9:697–701.
- Platonov AE, Karan LS, Kolyasnikova NM, Makhneva N, Toporkova MG, Maleev VV, Humans infected with the relapsing fever spirochete Borrelia miyamotoi, Russia. Emerg Infect Dis. 2011;17:1816–23.
- Gugliotta JL, Goethert HK, Berardi VP, Telford SR. Meningoencephalitis due to Borrelia miyamotoi in an elderly immunocompromised patient. N Engl J Med. 2013;368:240–5 .
- Krause PJ, Narasimhan S, Wormser GP, Rollend L, Fikrig E, Lepore T, Human Borrelia miyamotoi infection in the United States. N Engl J Med. 2013;368:291–3 .
- Chowdri HR, Gugliotta JL, Berardi V, Goethert H, Molloy PJ, Sterling SL, Borrelia miyamotoi presenting as human granulocytic anaplasmosis. A case report. Ann Intern Med. 2013;159:21–7.
- Hovius JW, de Wever B, Sohne M, Brouwer M, Coumou J, Wagemakers A, A case of meningoencephalitis by the relapsing fever spirochete Borrelia miyamotoi in Europe. Lancet. 2013;382:658.
- Sarksyan DS, Platonov AE, Karan LS, Malinin IE, Khaliltova LI, Shakhov VI, Clinical presentation of "new" tick-borne borreliosis caused by Borrelia miyamotoi [In Russian]. Ter Arkh. 2012;84:34–41 .
- Schwan TG, Schrumpf ME, Hinnebusch BJ, Anderson DE, Konkel ME. GlpQ: an antigen for serological discrimination between relapsing fever and Lyme borreliosis. J Clin Microbiol. 1996;34:2483–92 .
- Krause PJ, McKay K, Gadbaw J, Christianson D, Closter L, Lepore T, Increasing health burden of human babesiosis in endemic sites.Am J Trop Med Hyg. 2003;68:431–6 .
- Horowitz HW, Aguero-Rosenfeld ME, Holmgren D, McKenna D, Schwartz I, Cox ME, Lyme disease and human granulocytic anaplasmosis coinfection: impact of case definition on coinfection rates and illness severity. Clin Infect Dis. 2013;56:93–9 .
- Barbour AG, Jasinskas A, Kayala MA, Davies DH, Steere A, Baldi P, A genome-wide proteome array reveals a limited set of immunogens in natural infections of humans and white-footed mice with Borrelia burgdorferi. Infect Immun. 2008;76:3374–89 .
- Hue F, Ghalyanchi Langeroudi A, Barbour AG. Chromosome sequence of Borrelia miyamotoi, an uncultivable tick-borne agent of human infection. Genome Announc. 2013;1:e00713–13.
- Liang FT, Steere AC, Marques AR, Johnson BJ, Miller JN, Philipp MT. Sensitive and specific serodiagnosis of Lyme disease by enzyme-linked immunosorbent assay with a peptide based on an immunodominant conserved region of Borrelia burgdorferi VlsE. J Clin Microbiol. 1999;37:3990–6 .
- Magnarelli LA, Meegan JM, Anderson JF, Chappell WA. Comparison of an indirect fluorescent-antibody test with an enzyme-linked immunosorbent assay for serological studies of Lyme disease. J Clin Microbiol. 1984;20:181–4 .
- Dressler F, Whalen JA, Reinhardt BN, Steere AC. Western blotting in the serodiagnosis of Lyme disease. J Infect Dis. 1993;167:392–400.
- Bacon RM, Biggerstaff BJ, Schreifer M, Gilmore RD, Philipp MT, Steere AC, Serodiagnosis of Lyme disease by kinetic enzyme-linked immunosorbent assay using recombinant VlsE1 or peptide antigens of Borrelia burgdorferi compared with 2-tiered testing using whole-cell lysates. J Infect Dis. 2003;187:1187–99.
- Magnarelli LA, Anderson JF, Johnson RC. Cross-reactivity in serological tests for Lyme disease and other spirochetal infections. J Infect Dis. 1987;156:183–8.
- Magnarelli LA, Lawrenz M, Norris SJ, Fikrig E. Comparative reactivity of human sera to recombinant VlsE and other Borrelia burgdorferi antigens in class-specific enzyme-linked immunosorbent assays for Lyme borreliosis. J Med Microbiol. 2002;51:649–55 .
- Johnson ST, Cable RG, Tonnetti L, Spencer B, Rios J, Leiby DA. Seroprevalence of Babesia microti in blood donors from Babesia-endemic areas of the northeastern United States: 2000 through 2007. Transfusion. 2009;49:2574–82 .
- Krause PJ, Telford S, Spielman A, Sikand VJ, Ryan R, Christianson D, Concurrent Lyme disease and babesiosis: evidence for increased severity and duration of illness. JAMA. 1996;275:1657–60.
- Krause PJ, McKay K, Thompson CA, Sikand VJ, Lentz R, Lepore T, Disease-specific diagnosis of coinfecting tick-borne zoonoses: babesiosis, human granulocytic ehrlichiosis, and Lyme disease. Clin Infect Dis. 2002;34:1184–91.
- Ackermann R, Kabatzki J, Boisten HP, Steere AC, Grodzicki RL, Hartung S, Ixodes ricinus spirochete and European erythema chronicum migrans disease. Yale J Biol Med. 1984;57:573–80 .
- Centers for Disease Control and Prevention. Case definitions for infectious conditions under public health surveillance. MMWR Recomm Rep. 1997;46(RR-10):1–55 .
- Zhang JR, Hardham JM, Barbour AG, Norris SJ. Antigenic variation in Lyme disease borreliae by promiscuous recombination of VMP-like sequence cassettes. Cell. 1997;89:275–85.
- Salkeld DJ, Cinkovich S, Nieto NC. Tick-borne pathogens in northwestern California, USA [letter]. Emerg Infect Dis. 2014;20:493–4.
Figures
Tables
Cite This Article1Members of the Tick Borne Diseases Group are listed at the end of this article.




















.png)


.png)










No hay comentarios:
Publicar un comentario