Chronic Kidney Disease in the United States, 2019
Download the print version: Chronic Kidney Disease in the United States, 2019 [PDF – 2 MB]
With chronic kidney disease (CKD), kidneys become damaged over time or cannot clean the blood as well as healthy kidneys. When the kidneys don’t work well, wastes and extra water build up in the body and may cause other health problems, including heart disease and high blood pressure. However, people with CKD and people at risk for CKD can take steps to protect their kidneys.
CKD Is Common Among US Adults

Fast Stats
- 15% of US adults—37 million people—are estimated to have CKD.*
- Most (9 in 10) adults with CKD do not know they have it.
- 1 in 2 people with very low kidney function who are not on dialysis do not know they have CKD.
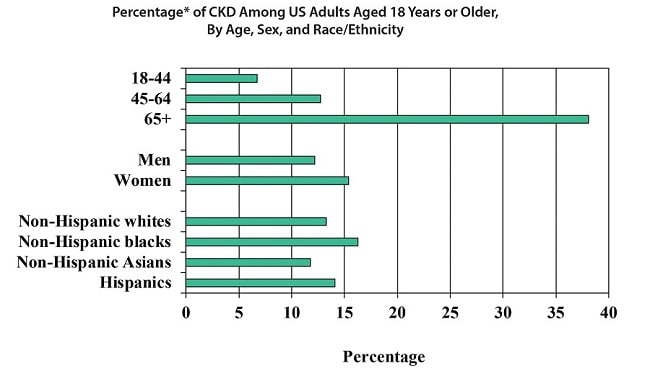
According to current estimates:*
- CKD is more common in people aged 65 years or older (38%) than in people aged 45–64 years (13%) or 18–44 years (7%).
- CKD is more common in women (15%) than men (12%).
- CKD is more common in non-Hispanic blacks (16%) than in non-Hispanic whites (13%) or non-Hispanic Asians (12%).
- About 14% of Hispanics have CKD.
CKD Risk Factors
Diabetes and high blood pressure are the major causes of CKD in adults. Other risk factors include heart disease, obesity, a family history of CKD, past damage to the kidneys, and older age.
Keep kidneys healthy
by managing blood sugar and
blood pressure.
by managing blood sugar and
blood pressure.
Ways to Prevent CKD or Detect It Early
- Control risk factors for CKD:
- High blood pressure.
- High blood sugar levels.
Keeping a healthy body weight through a balanced diet and physical activity may help.
- Test for CKD regularly in people who have diabetes, high blood pressure, or other risk factors for CKD.
Testing and Treatment
- People may not feel ill or notice any symptoms until CKD is advanced.
- The only way to find out if people have CKD is through simple blood and urine tests. The blood test checks for creatinine (a waste product produced by muscles) in the blood to see how well the kidneys work. The urine test checks for protein in the urine (a sign of kidney damage).
- Following a healthy diet and taking medicine for diabetes and high blood pressure may keep CKD from getting worse and may prevent other health problems such as heart disease.
CKD-Related Health Problems
Early Death
Adults with CKD are at a higher risk of early death compared to adults without CKD of the same age.
Heart Disease and Stroke
- Having CKD increases the chances of also having heart disease and stroke.
- Managing high blood pressure, blood sugar, and cholesterol levels—all factors that increase the risk for heart disease and stroke—is very important for people with CKD.
Other Health Problems
As CKD worsens over time related health problems become more likely, including:
- Anemia or low red blood cell count (can cause fatigue and weakness).
- Low calcium levels and high phosphorus levels in the blood (can cause bone problems).
- High potassium levels in the blood (can cause an irregular or abnormal heartbeat).
- Loss of appetite or nausea.
- Extra fluid in the body (can cause high blood pressure, swelling in the legs, or shortness of breath).
- Infections or a weakened immune system.
- Depression.
Kidney Failure
If kidney damage is severe and kidney function is very low, dialysis or a kidney transplant is needed for survival. Kidney failure treated with dialysis or a kidney transplant is called end-stage kidney disease (ESKD). Treatment may slow the decline in kidney function and delay kidney failure. However, not everyone with CKD develops ESKD, and in some cases ESKD develops even with treatment.
Facts About ESKD
- In 2016, nearly 125,000 people in the United States started treatment for ESKD, and more than 726,000 (2 in every 1,000 people) were on dialysis or were living with a kidney transplant.
- Every day, more than 240 people on dialysis die.
- For every 2 women who develop ESKD, 3 men develop ESKD.
- African Americans are about 3 times more likely than whites to develop ESKD.
- For every 3 non-Hispanics who develop ESKD, 4 Hispanics develop ESKD.
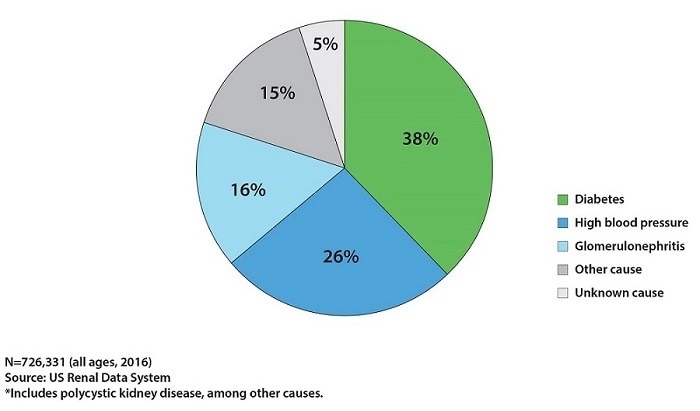
- In US adults aged 18 years or older, diabetes and high blood pressure are the main reported causes of ESKD.
- In US children and adolescents younger than 18 years, polycystic kidney disease and glomerulonephritis (inflammation of the kidneys) are the main causes of ESKD.
Reported Causes of End-stage Kidney Disease
in the United States
in the United States
People With CKD Can Lower Their Risk for Kidney Failure
- Learn about CKD from their kidney doctor (nephrologist) to better understand treatment and protect their kidneys. People with nephritis, polycystic kidney disease (a cause of CKD and kidney failure), or other kidney disease should talk about specific treatment options with their kidney doctor.
- Manage blood sugar and blood pressure.
- Manage CKD:
- Make lifestyle changes (e.g., healthy eating, exercise) to prevent more kidney damage. Meet with a dietitian to create a kidney-healthy eating plan that is low in salt and fat and has the right amount of protein. As CKD gets worse, the plan may also include limiting phosphorus and potassium.
- Use medicines (e.g., drugs to lower blood pressure) to slow the decline in kidney function.
- Stop smoking.
- Avoid conditions or exposures that can harm the kidneys or cause kidney function to suddenly get worse:
- Certain medicines:
- Over-the-counter pain medicines like ibuprofen and naproxen.
- Some antibiotics.
- Proton pump inhibitors used to reduce stomach acid, such as omeprazole and lansoprazole.
- Herbal supplements (always talk to your doctor before taking any supplements).
- Certain dyes (contrast agents) used to make blood vessels or organs visible on X-rays or other imaging tests.
- Kidney infections (preventing bladder infections may help).
- Certain medicines:
- Check with a doctor about other things to avoid.
People with diabetes, high blood pressure, or CKD should
talk to their doctor about how to protect their kidneys.
talk to their doctor about how to protect their kidneys.



*Percentage of CKD stages 1–4 among US adults aged 18 years or older using data from the 2013–2016 National Health and Nutrition Examination Survey and the CKD Epidemiology Collaboration (CKD-EPI) equation. These estimates were based on a single measure of albuminuria or serum creatinine; they do not account for persistence of albuminuria or creatinine as indicated by the Kidney Disease Improving Global Outcomes recommendations. Thus, CKD in this report might be overestimated. Estimates by sex and race/ethnicity were age-standardized using the 2000 US census population; the overall percentage is unadjusted. The number of adults with CKD stages 1–4 was estimated by applying the overall percentage to the 2016 US Census population.
Acknowledgments
The following organizations** collaborated in developing and reviewing this fact sheet:
- Centers for Disease Control and Prevention
- US Department of Defense
- US Department of Veterans Affairs
- Kidney Interagency Coordinating Committee
- National Heart, Lung, and Blood Institute of the National Institutes of Health
- National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health
- United States Renal Data System
- National Kidney Disease Education Program
- American Society of Nephrology
- National Kidney Foundation
- University of California, San Francisco, and University of California, San Francisco Center for Vulnerable Populations
- University of Michigan, Division of Nephrology, Department of Internal Medicine, and University of Michigan Kidney Epidemiology and Cost Center
**Links to nonfederal organizations are provided solely as a courtesy. Links do not constitute an endorsement of any organization by CDC or the federal government, and none should be inferred. CDC is not responsible for the content of the individual organization’s web pages.
Note
This publication is not subject to copyright restrictions; duplicate and distribute copies as desired.
Citation
Centers for Disease Control and Prevention. Chronic Kidney Disease in the United States, 2019. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention; 2019.
References
- Centers for Disease Control and Prevention. Chronic Kidney Disease Surveillance System website. https://nccd.cdc.gov/CKD. Accessed January 7, 2019.
- Kidney Disease: Improving Global Outcomes CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Inter. 2013;3(1)(suppl):1–150.
- Meisinger C, Döring A, Löwel H, KORA Study Group. Chronic kidney disease and risk of incident myocardial infarction and all-cause and cardiovascular disease mortality in middle-aged men and women from the general population. Eur Heart J. 2006;27(10):1245–1250.
- National Institutes of Health. 2018 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2018.
- Astor BC, Hallan SI, Miller ER 3rd, Yeung E, Coresh J. Glomerular filtration rate, albuminuria, and risk of cardiovascular and all-cause mortality in the U.S. population. Am J Epidemiol. 2008;167(10):1226–1234.
- Hemmelgarn BR, James MT, Manns BJ, et al. Rates of treated and untreated kidney failure in older vs younger adults. JAMA. 2012;307(23):2507–2715.
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296–1305.
- Yarnoff BO, Hoerger TJ, Shrestha SS, et al. Modeling the impact of obesity on the lifetime risk of chronic kidney disease in the United States using updated estimates of GFR progression from the CRIC study. PLoS One. 2018;13(10):e0205530.
- Perlman RL, Finkelstein FO, Liu L, et al. Quality of life in chronic kidney disease (CKD): a cross-sectional analysis in the Renal Research Institute-CKD study. Am J Kidney Dis. 2005;45(4):658–666.
- Kinchen KS, Sadler J, Fink N, et al. The timing of specialist evaluation in chronic kidney disease and mortality. Ann Intern Med. 2002;137(6):479–486.
- Burrows NR, Vassalotti JA, Saydah SH, et al. Identifying high-risk individuals for chronic kidney disease: results of the CHERISH Community Demonstration Project. Am J Nephrol. 2018;48(6):447–455.
- Snyder JJ, Collins AJ. Association of preventive health care with atherosclerotic heart disease and mortality in CKD. J Am Soc Nephrol. 2009;20(7):1614–1622.
- Hoerger TJ, Wittenborn JS, Segel JE, et al. A health policy model of CKD: 2. The cost-effectiveness of microalbuminuria screening. Am J Kidney Dis. 2010;55(3):463–473.
- National Institutes of Health. Health Information: Chronic Kidney Disease website. https://www.niddk.nih.gov/health-information/kidney-disease/chronic-kidney-disease-ckd. Accessed February 7, 2019.
For Public Inquiries and Publications
CDC-INFO Contact Center
Telephone: 1-800-CDC-INFO (232-4636)
1-888-232-6348 TTY
E-Mail: cdcinfo@cdc.gov
In English and Spanish
24 hours a day, 7 days a week
1-888-232-6348 TTY
E-Mail: cdcinfo@cdc.gov
In English and Spanish
24 hours a day, 7 days a week
For Other Information
Division of Diabetes Translation
National Center for Chronic Disease Prevention and Health Promotion
Centers for Disease Control and Prevention
4770 Buford Highway NE, Mailstop F-75, Atlanta, GA 30341-3717
Telephone 770-488-5000; Fax 770-488-8211
National Center for Chronic Disease Prevention and Health Promotion
Centers for Disease Control and Prevention
4770 Buford Highway NE, Mailstop F-75, Atlanta, GA 30341-3717
Telephone 770-488-5000; Fax 770-488-8211























.png)










No hay comentarios:
Publicar un comentario