Aporte a la rutina de la trinchera asistencial donde los conocimientos se funden con las demandas de los pacientes, sus necesidades y las esperanzas de permanecer en la gracia de la SALUD.
MedWatch - The FDA Safety Information and Adverse Event Reporting Program
Keytruda (pembrolizumab) in Patients with Multiple Myeloma: FDA Statement - Two Clinical Trials on Hold
AUDIENCE: Oncology
ISSUE: Based on data from two recently halted clinical trials, the U.S. Food and Drug Administration today is issuing this statement to inform the public, health care professionals, and oncology clinical investigators about the risks associated with the use of Keytruda (pembrolizumab) in combination with dexamethasone and an immunomodulatory agent (lenalidomide or pomalidomide) for the treatment of patients with multiple myeloma. Keytruda (pembrolizumab) is not approved for treatment of multiple myeloma.
The FDA statement is based on review of data from two clinical trials (KEYNOTE-183 and KEYNOTE-185) evaluating the use of Keytruda (pembrolizumab) combined with other treatments in patients with multiple myeloma. On July 3, 2017, the FDA required that all patients in these trials be discontinued from further investigation with this drug, because interim results from both trials demonstrated an increased risk of death for patients receiving Keytruda (pembrolizumab) when it was combined with an immunomodulatory agent as compared to the control group (see statistical analysis section below). Merck & Co., Inc. was made aware of the issue through an external data monitoring committee recommendation and suspended the trials to enrollment on June 12, 2017. BACKGROUND: This does not apply to patients taking Keytruda (pembrolizumab) for an approved indication. Patients on Keytruda (pembrolizumab) for an approved use should continue to take their medication as directed by their health care professional.
Keytruda (pembrolizumab) is currently approved by the FDA for treatment of: Melanoma, Lung Cancer, Head and Neck Cancer, Classical Hodgkin Lymphoma, Urothelial Carcinoma, Microsatellite Instability-High (MSI-H) Cancer.
For a summary of the statistical analysis and findings, please refer to the FDA Statement.
RECOMMENDATION: Other multiple myeloma clinical trials of Keytruda (pembrolizumab), other PD-1/PD-L1 cancer drugs and other combinations are currently undergoing clinical evaluation. The FDA will be working directly with sponsors of Keytruda and other PD-1/PD-L1 cancer drugs, as well as clinical investigators conducting clinical trials in patients with multiple myeloma, to determine the extent of the safety issue. The agency will communicate any new information to the public as soon as it is able.
Health care professionals and consumers are encouraged to report any adverse events or side effects related to the use of these products and other similar products to FDA’s MedWatch Adverse Event Reporting program:
Download form or call 1-800-332-1088 to request a reporting form, then complete and return to the address on the pre-addressed form, or submit by fax to 1-800-FDA-0178
Bringing the Investigational Breast Cancer Drug Endoxifen from Bench to Bedside with NCI Support
August 31, 2017, by Matthew Goetz, M.D.
Many stories of successful cancer research follow a familiar arc: one of curiosity, iteration, collaboration, and persistence. The development of endoxifen, an investigational drug for breast cancer, is no different.
Like many research advances, the endoxifen story started with intriguing basic research findings that the research community continuously expanded on, eventually leading to clinical trials.
But this progress, and that of many other cancer research projects, was dependent on a critical component: endoxifen’s development would not have been possible without the support of NCI, as well as other government, nonprofit, and philanthropic organizations.
Tamoxifen blocks breast cancer cell growth by preventing estrogen from binding to estrogen receptors (ERs). Many women with ER-positive breast cancer are treated with tamoxifen, and it’s estimated that the treatment has saved the lives of half a million women around the world.
But the efficacy of tamoxifen treatment varies and the drug does not work at all for about one-third of women with ER-positive breast cancer.
There likely are several reasons for this variability, and more than a decade ago, our research team at the Mayo Clinic hypothesized that one contributing factor may be how tamoxifen is processed in the body.
Tamoxifen binds only weakly to ERs, but can undergo a processing step inside the body to gain more potent anticancer activity. This step happens in the liver, where a series of enzymes, including one called CYP2D6, modifies tamoxifen to create other compounds. Two of these compounds—endoxifen and 4-hydroxy tamoxifen—inhibit estrogen up to 100 times more strongly than tamoxifen.
More than 100 common genetic alterations, called polymorphisms, in the CYP2D6 gene have been identified, and some of these alterations reduce CYP2D6’s enzyme activity. At the time our team began this research project, however, the impact of these genetic alterations on tamoxifen’s efficacy was unknown.
At that time, a research group led by David Flockhart, M.D., Ph.D., at Indiana University demonstrated that, among tamoxifen-treated women, those with low CYP2D6 activity—due to having a low-activity polymorphism or taking medications that block the enzyme—had lower levels of endoxifen in their blood compared with women with normal enzyme activity.
In 2005, with funding from an NCI grant, we collaborated with Dr. Flockhart’s group to analyze CYP2D6 polymorphisms in 223 women who had previously participated in an NCI-funded trial of tamoxifen. We found that patients with polymorphisms that lower CYP2D6 activity were more likely to relapse after tamoxifen treatment than patients with normal CYP2D6 activity.
With additional funding from NCI, we verified these findings in a second study of 1,325 women with breast cancer and a meta-analysis within the International Tamoxifen Pharmacogenomics Consortium.
We later discovered that endoxifen is critical for tamoxifen’s anticancer effects. In our lab experiments, for example, higher endoxifen concentrations (like those achieved in patients with high CYP2D6 activity) resulted in greater inhibition of breast cancer cell growth than low endoxifen concentrations (such as those observed in patients with low CYP2D6 activity).
Similarly, a separate group of investigators found that endoxifen halted the growth in five of the six breast cancer cell lines in the NCI-60 Human Tumor Cell Lines Screen. They found that endoxifen also slowed the growth of human breast cancer tumors in mice.
With this evidence, it became clear that tamoxifen treatment may be less effective for some women with low CYP2D6 activity simply because they produce less endoxifen. So, we thought, what if we could bypass CYP2D6 altogether by treating patients with endoxifen instead of tamoxifen?
To explore this idea, several members of the Mayo team performed experiments in lab animals to determine endoxifen’s pharmacokinetics—that is, how the drug is absorbed, distributed, and excreted. Endoxifen had a good profile by these measures, boosting its potential as a drug candidate.
For many of these preclinical studies, our team was supported by a Specialized Programs of Research Excellence (SPORE) grant, an NCI program that is designed to rapidly translate basic science discoveries into clinical applications. Igor Kuzmin, Ph.D., a program director in NCI’s Translational Research Program who manages the Mayo Clinic’s breast cancer SPORE, helped guide our endoxifen project from a small idea into a potential drug candidate.
Transitioning Endoxifen to Clinical Trials
Our next step was to develop endoxifen into a drug that could be administered to humans. But because its chemical structure was already public knowledge, there was limited interest in its drug development by pharmaceutical companies.
NCI, however, was in a position to step in again. As a part of its broad mission to bolster cancer research, NCI is uniquely qualified to develop promising new treatments or drugs that have limited potential for commercialization.
The institute recognized the potential of endoxifen to fill an important niche in the treatment of breast cancer, and with the help of NCI’s Developmental Therapeutics Program, led by Jerry Collins, Ph.D., endoxifen was formulated and synthesized for human treatment. Together, Mayo and NCI researchers further evaluated the safety of endoxifen in larger, more robust laboratory studies.
With promising results from these preclinical studies, NCI filed an Investigational New Drug application for endoxifen with the Food and Drug Administration (FDA) so that clinical trials could begin.
In one of the trials, we achieved the major goal of attaining the desired concentration of endoxifen independent of patients’ CYP2D6 activity. In addition, we observed encouraging antitumor activity, including in women whose tumors had progressed on tamoxifen, aromatase inhibitors, and the estrogen receptor inhibitor fulvestrant (Faslodex®).
In 2015, we initiated a randomized phase II trial comparing how well endoxifen and tamoxifen work in women with breast cancer, with results expected in early 2018. The trial is sponsored by NCI’s Cancer Therapy Evaluation Program and is conducted by the Alliance for Clinical Trials in Oncology, an NCI-funded clinical trials group.
A Needed Treatment Option
Matthew Goetz, M.D. Professor of Oncology and Pharmacology Mayo Clinic Rochester, Minnesota
There is a major need for a better treatment option for the 5% to 20% of women diagnosed annually with ER-positive breast cancer for whom tamoxifen is ineffective, and direct endoxifen treatment may address that need.
If endoxifen shows promise in these trials, NCI could collaborate with an industry partner to manufacture it on a large scale and possibly move the investigational drug into the larger trials needed for FDA approval. If approved, a genetic test could potentially identify patients who are most (and least) likely to benefit from tamoxifen or endoxifen treatment.
It’s not yet clear how this endoxifen story will end. Drug development is costly and time consuming, and there’s no way to know if a drug will benefit patients until it is rigorously tested in multiple clinical trials.
What is clear, however, is that without the commitment and collaborative spirit of the Mayo team—including James Ingle, M.D., Matthew Ames, Ph.D., Joel Reid, Ph.D., Thomas Spelsberg, Ph.D., and John Hawse, Ph.D.—and NCI’s continuous support, this potentially promising therapy might never have been developed. I’m thankful to have come this far with our story, and am hopeful that our efforts will ultimately lead to beneficial results for patients.
Modified Stem Cells Deliver Chemotherapy to Metastatic Tumors
August 30, 2017, by NCI Staff
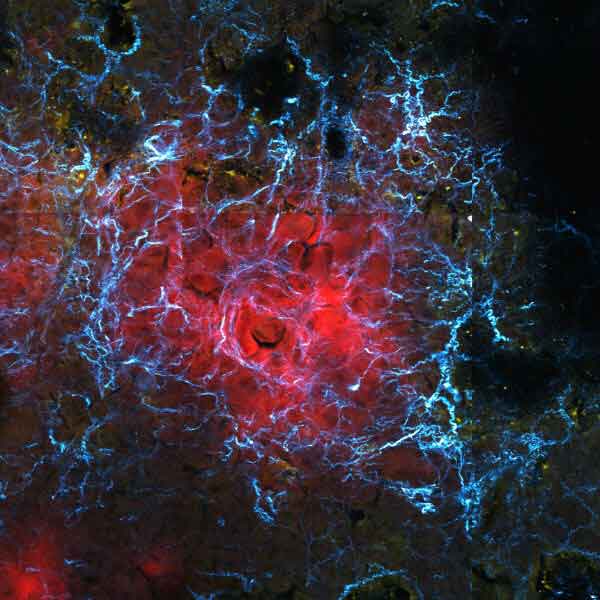
Researchers have developed a treatment that targets stiff components of the extracellular matrix (blue) surrounding metastatic cancer cells (red) as a potential therapy for metastatic cancer.
Credit: Jenu Chacko, Ph.D. and Linan Liu, Ph..D., University of California, Irvine
Researchers have used modified stem cells to deliver a cancer drug selectively to metastatic breast cancer tumors in mice. The stem cells specifically targeted metastatic tumors by homing in on the stiff environment that typically surrounds them.
Compared with nonmodified stem cells, the modified stem cell treatment shrank metastatic breast tumors in mice and improved their rate of survival. The study results were published July 26 in Science Translational Medicine.
Components in the area surrounding tumors, called the tumor microenvironment, can directly affect cancer progression and metastasis. Now, the research team believes, they may have found a way to take advantage of the tumor microenvironment.
In contrast to other therapies that target cancer cells directly, “we demonstrated that you can actually target the ‘home’ where cancer cells reside—the tumor microenvironment,” said the study’s lead investigator, Weian Zhao, Ph.D., of University of California, Irvine.
“The concept of the study is novel and very promising therapeutically. It is a great proof of principle. Although there remains a lot of details to work out, it has the potential to change the way we treat patients at high risk for metastasis,” said Rosandra Kaplan, M.D., head of the Tumor Microenvironment Section of NCI’s Center for Cancer Research, who was not involved in the study.
An exciting characteristic of the approach, Dr. Kaplan continued, is that it is adjustable and dynamic, which means that it may potentially be fine-tuned to an individual patient’s needs.
“When you give a patient a big whopping dose of chemotherapy, it’s like a bomb,” she said. “This is more like Navy Seal stealth action, like knowing what position to get in and exactly when to pull the trigger. There’s a lot of promise there.”
A Stiff Microenvironment
Although metastatic cancer accounts for the majority of cancer deaths, no currently available cancer treatment specifically targets metastatic tumors. Dr. Zhao and his colleagues wondered whether specific components of the tumor microenvironment might allow them to zero in on metastatic tumors.
Within the tumor microenvironment, a latticework of fibrous molecules called the extracellular matrix provides a “foundation for cells to communicate information with each other and a set of train tracks, if you will, for them to move on,” explained Dr. Kaplan. In addition, the physical stiffness of the matrix can influence the behavior of nearby cells.
For example, when breast cancer cells metastasize, they tend to settle in stiff extracellular matrices in the lungs. Signals and cues from the extracellular matrix help the cancer cells survive and grow in their new environment, she continued.
A stiff matrix in the microenvironment can also affect gene expression and development of a kind of adult stem cell, called mesenchymal stem cells (MSCs), which helps repair injured tissues. Specifically, if these stem cells—which can develop into several different cell types—encounter a more rigid matrix, they become bone cells. But if they are in in a more flexible matrix, they turn into fat cells.
In addition, MSCs preferentially settle near tumors, and some researchers think that the stiff microenvironment may help recruit them.
Because of the properties of MSCs, Dr. Zhao and his team reasoned that these cells might be used to specifically target tumors. While the researchers focused on metastatic tumors in their current study, their approach could theoretically “target primary tumors as well,” Dr. Zhao said.
To manipulate MSCs into delivering cancer therapy to tumors, the researchers modified the cells so that they would express the gene for a key enzyme only when they encounter a stiff microenvironment. The enzyme, called cytosine deaminase (CD), converts the chemical flucytosine into the chemotherapy drug fluorouracil.
Fluorouracil is commonly used to treat breast cancer. But like other chemotherapy drugs, it can damage healthy tissues and lead to toxicity when given systemically.
The team’s hope was that by modifying MSCs to express the CD enzyme only in the stiff tumor microenvironment, the chemotherapy drug would be activated specifically near tumors, preferentially killing cancer cells while sparing healthy cells.
Targeting Metastatic Tumors
In lab experiments, the researchers mixed the modified MSCs, breast cancer cells, and flucytosine on different surfaces. They found that the modified MSCs expressed CD and reduced breast cancer cell growth when placed on a stiff glass surface but not when placed on a soft gel surface.
Next, they implanted mice with human breast cancer cells, which eventually formed metastatic tumors in the mice’s lungs. They then injected these mice with the modified or nonmodified MSCs, and, the following day, injected them with flucytosine.
The modified MSCs homed to metastatic lung tumors and expressed CD, the researchers found, and the activated flucytosine reduced tumor size and improved survival of the mice. There was no effect, however, on tumor size or survival in mice treated with nonmodified MSCs and flucytosine.
In addition, they found that the modified MSCs did not damage healthy cells in the bone marrow, livers, or brains of mice. But when they injected mice with MSCs that constantly expressed CD, followed by an injection of flucytosine, the treatment damaged healthy tissue.
This is presumably because flucytosine was activated outside of the tumor, and it demonstrates that a targeted approach is critical to reducing its harmful side effects, Dr. Zhao said.
Dr. Kaplan said, “it’s clear that they have a means to deliver chemotherapy with potentially less toxicity, but it still may cause local toxicity,” meaning it damaged healthy tissue in the area near the tumor. Another concern, she added, is that not all tumors may be sensitive to the effects of fluorouracil.
In addition, how the immune system may interact with these modified MSCs remains an open question, Dr. Kaplan noted.
“We know that, in general, cell-based therapies can be fraught with immune-related issues, such as elimination of modified cells by immune cells.”
Taking Advantage of the Microenvironment
Unmodified MSCs are currently being tested in over 100 clinical trials as experimental therapies for different diseases, including cancer, and so far have proven to be safe in humans.
The stem cells are typically collected from the bone marrow, fat, or umbilical cord tissue of a patient or an unrelated donor. So unlike other cell-based therapies, MSC-based therapies don’t require a personalized treatment for each individual patient, said Dr. Zhao. Rather, an off-the-shelf treatment for hundreds of patients can be created from MSCs obtained from a single unrelated donor, he explained.
Looking forward, the research team has NCI funding to try incorporating their approach into a type of immunotherapy called CAR T-cell therapy. While CAR T-cell therapy is a promising experimental cancer treatment, it can cause severe—sometimes life-threatening—side effects by unintentionally damaging healthy tissues.
“We are working to create CAR T-cells that not only recognize the tumor but that also have to recognize the tumor microenvironment before they activate their killing mechanism,” Dr. Zhao said. “This way, we make sure they are not just effective but safe as well.”
Researchers and others gather at the National Cancer Institute's exhibit booth during the 2017 American Association for Cancer Research (AACR) annual meeting in Washington, D.C.
Researchers and others gather at the National Cancer Institute's exhibit booth during the 2017 American Association for Cancer Research (AACR) annual meeting in Washington, D.C.
Researchers and others gather at the National Cancer Institute's exhibit booth during the 2017 American Association for Cancer Research (AACR) annual meeting in Washington, D.C.
Researchers and others gather at the National Cancer Institute's exhibit booth during the 2017 American Association for Cancer Research (AACR) annual meeting in Washington, D.C.
Researchers and others gather at the National Cancer Institute's exhibit booth during the 2017 American Association for Cancer Research (AACR) annual meeting in Washington, D.C.
Researchers and others gather at the National Cancer Institute's exhibit booth during the 2017 American Association for Cancer Research (AACR) annual meeting in Washington, D.C.
Researchers and others gather at the National Cancer Institute's exhibit booth during the 2017 American Association for Cancer Research (AACR) annual meeting in Washington, D.C.
Researchers and others gather at the National Cancer Institute's exhibit booth during the 2017 American Association for Cancer Research (AACR) annual meeting in Washington, D.C.
Researchers and others gather at the National Cancer Institute's exhibit booth during the 2017 American Association for Cancer Research (AACR) annual meeting in Washington, D.C.
Researchers and others gather at the National Cancer Institute's exhibit booth during the 2017 American Association for Cancer Research (AACR) annual meeting in Washington, D.C.
Researchers and others gather at the National Cancer Institute's exhibit booth during the 2017 American Association for Cancer Research (AACR) annual meeting in Washington, D.C.
Researchers and others gather at the National Cancer Institute's exhibit booth during the 2017 American Association for Cancer Research (AACR) annual meeting in Washington, D.C.
Researchers and others gather at the National Cancer Institute's exhibit booth during the 2017 American Association for Cancer Research (AACR) annual meeting in Washington, D.C.
Researchers and others gather at the National Cancer Institute's exhibit booth during the 2017 American Association for Cancer Research (AACR) annual meeting in Washington, D.C.
Researchers and others gather at the National Cancer Institute's exhibit booth during the 2017 American Association for Cancer Research (AACR) annual meeting in Washington, D.C.